

CT imaging post-TAVI: Murphy's first law in action-preparing to recognize the unexpected
- PMID: 38900378
- PMCID: PMC11189851
- DOI: 10.1186/s13244-024-01729-1
CT imaging post-TAVI: Murphy's first law in action-preparing to recognize the unexpected
Abstract
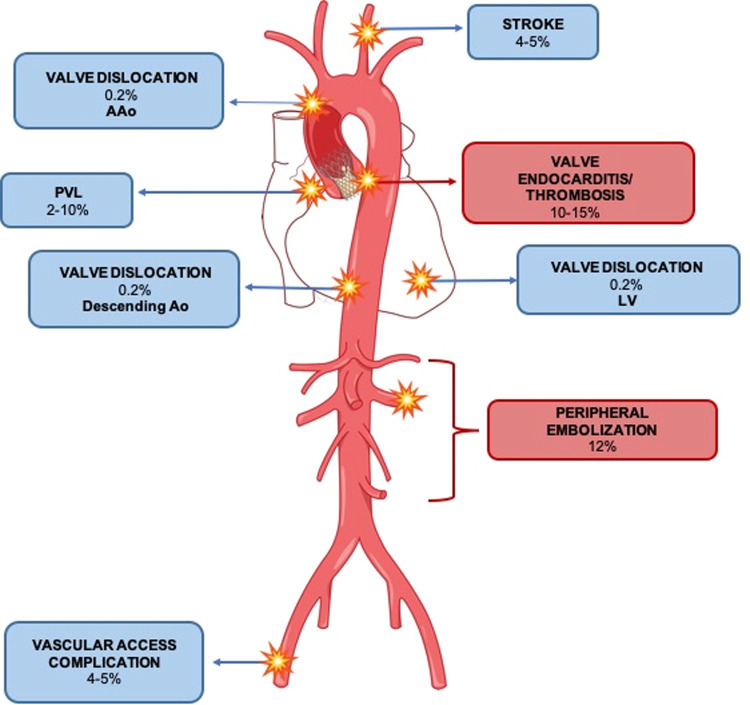
Transfemoral aortic valve implantation (TAVI) has been long considered the standard of therapy for high-risk patients with severe aortic-stenosis and is now effectively employed in place of surgical aortic valve replacement also in intermediate-risk patients. The potential lasting consequences of minor complications, which might have limited impact on elderly patients, could be more noteworthy in the longer term when occurring in younger individuals. That's why a greater focus on early diagnosis, correct management, and prevention of post-procedural complications is key to achieve satisfactory results. ECG-triggered multidetector computed tomography angiography (CTA) is the mainstay imaging modality for pre-procedural planning of TAVI and is also used for post-interventional early detection of both acute and long-term complications. CTA allows detailed morphological analysis of the valve and its movement throughout the entire cardiac cycle. Moreover, stent position, coronary artery branches, and integrity of the aortic root can be precisely evaluated. Imaging reliability implies the correct technical setting of the computed tomography scan, knowledge of valve type, normal post-interventional findings, and awareness of classic and life-threatening complications after a TAVI procedure. This educational review discusses the main post-procedural complications of TAVI with a specific imaging focus, trying to clearly describe the technical aspects of CTA Imaging in post-TAVI and its clinical applications and challenges, with a final focus on future perspectives and emerging technologies. CRITICAL RELEVANCE STATEMENT: This review undertakes an analysis of the role computed tomography angiography (CTA) plays in the assessment of post-TAVI complications. Highlighting the educational issues related to the topic, empowers radiologists to refine their clinical approach, contributing to enhanced patient care. KEY POINTS: Prompt recognition of TAVI complications, ranging from value issues to death, is crucial. Adherence to recommended scanning protocols, and the optimization of tailored protocols, is essential. CTA is central in the diagnosis of TAVI complications and functions as a gatekeeper to treatment.
Keywords: Cardiac imaging; Complications; Computed tomography angiography (CTA); Transfemoral aortic valve implantation (TAVI).
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Vahanian A, Beyersdorf F, Praz F, et al. 2021 ESC/EACTS guidelines for the management of valvular heart disease: developed by the task force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) Rev Esp Cardiol (Engl Ed) 2022;75:524. doi: 10.1016/j.rec.2022.05.006. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
