

Predictors of mortality of Pseudomonas aeruginosa bacteraemia and the role of infectious diseases consultation and source control; a retrospective cohort study
- PMID: 38900392
- PMCID: PMC11825531
- DOI: 10.1007/s15010-024-02326-6
Predictors of mortality of Pseudomonas aeruginosa bacteraemia and the role of infectious diseases consultation and source control; a retrospective cohort study
Abstract
Purpose: To determine predictors of mortality among patients with Pseudomonas aeruginosa bacteraemia.
Methods: Retrospective study.
Setting: This study conducted at the Lausanne University Hospital, Switzerland included adult patients with P. aeruginosa bacteraemia from 2015 to 2021.
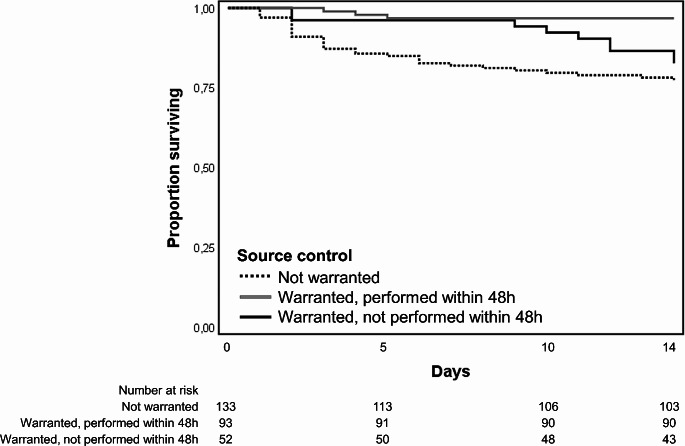
Results: During the study period, 278 episodes of P. aeruginosa bacteraemia were included. Twenty (7%) isolates were multidrug-resistant. The most common type of infection was low respiratory tract infection (58 episodes; 21%). Sepsis was present in the majority of episodes (152; 55%). Infectious diseases consultation within 48 h of bacteraemia onset was performed in 203 (73%) episodes. Appropriate antimicrobial treatment was administered within 48 h in 257 (92%) episodes. For most episodes (145; 52%), source control was considered necessary, with 93 (64%) of them undergoing such interventions within 48 h. The 14-day mortality was 15% (42 episodes). The Cox multivariable regression model showed that 14-day mortality was associated with sepsis (P 0.002; aHR 6.58, CI 1.95-22.16), and lower respiratory tract infection (P < 0.001; aHR 4.63, CI 1.78-12.06). Conversely, interventions performed within 48 h of bacteraemia onset, such as infectious diseases consultation (P 0.036; HR 0.51, CI 0.27-0.96), and source control (P 0.009; aHR 0.17, CI 0.47-0.64) were associated with improved outcome.
Conclusion: Our findings underscore the pivotal role of early infectious diseases consultation in recommending source control interventions and guiding antimicrobial treatment for patients with P. aeruginosa bacteraemia.
Keywords: Pseudomonas aeruginosa; Infectious diseases consultation; Multidrug resistance; Sepsis; Source control.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Statements and Declarations: A part of this work was presented at the 34th European Congress of Clinical Microbiology and Infectious Diseases on 27–30 April 2024 in Barcelona, Spain. Ethics approval: The study adhered to the Declaration of Helsinki and was approved by the ethics committee of the Canton of Vaud (CER-VD 2021–02516). Consent to participate: Due to the retrospective nature of the study, the ethic committee waived the need of informed consent to participate. However, patients were excluded if they had previously refused to permit the use of their data for research purposes. Consent to publish: Due to the retrospective nature of the study, the ethic committee waived the need of informed consent to publish. However, patients were excluded if they had previously refused to permit the use of their data for research purposes. Competing interests: The authors declare no competing interests.
Figures
References
-
- Thaden JT, Park LP, Maskarinec SA, Ruffin F, Fowler VG Jr., van Duin D. Results from a 13-Year prospective cohort study show increased Mortality Associated with Bloodstream infections caused by Pseudomonas aeruginosa compared to other Bacteria. Antimicrob Agents Chemother. 2017;61(6). 10.1128/AAC.02671-16. - PMC - PubMed
-
- Kang CI, Kim SH, Kim HB, Park SW, Choe YJ, Oh MD, et al. Pseudomonas aeruginosa bacteremia: risk factors for mortality and influence of delayed receipt of effective antimicrobial therapy on clinical outcome. Clin Infect Diseases: Official Publication Infect Dis Soc Am. 2003;37(6):745–51. 10.1086/377200. - PubMed
-
- Zhen S, Zhao Y, Chen Z, Zhang T, Wang J, Jiang E, et al. Assessment of mortality-related risk factors and effective antimicrobial regimens for treatment of bloodstream infections caused by carbapenem-resistant Pseudomonas aeruginosa in patients with hematological diseases. Front Cell Infect Microbiol. 2023;13:1156651. 10.3389/fcimb.2023.1156651. - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
