

JAK inhibition enhances checkpoint blockade immunotherapy in patients with Hodgkin lymphoma
- PMID: 38900864
- PMCID: PMC11283877
- DOI: 10.1126/science.ade8520
JAK inhibition enhances checkpoint blockade immunotherapy in patients with Hodgkin lymphoma
Abstract
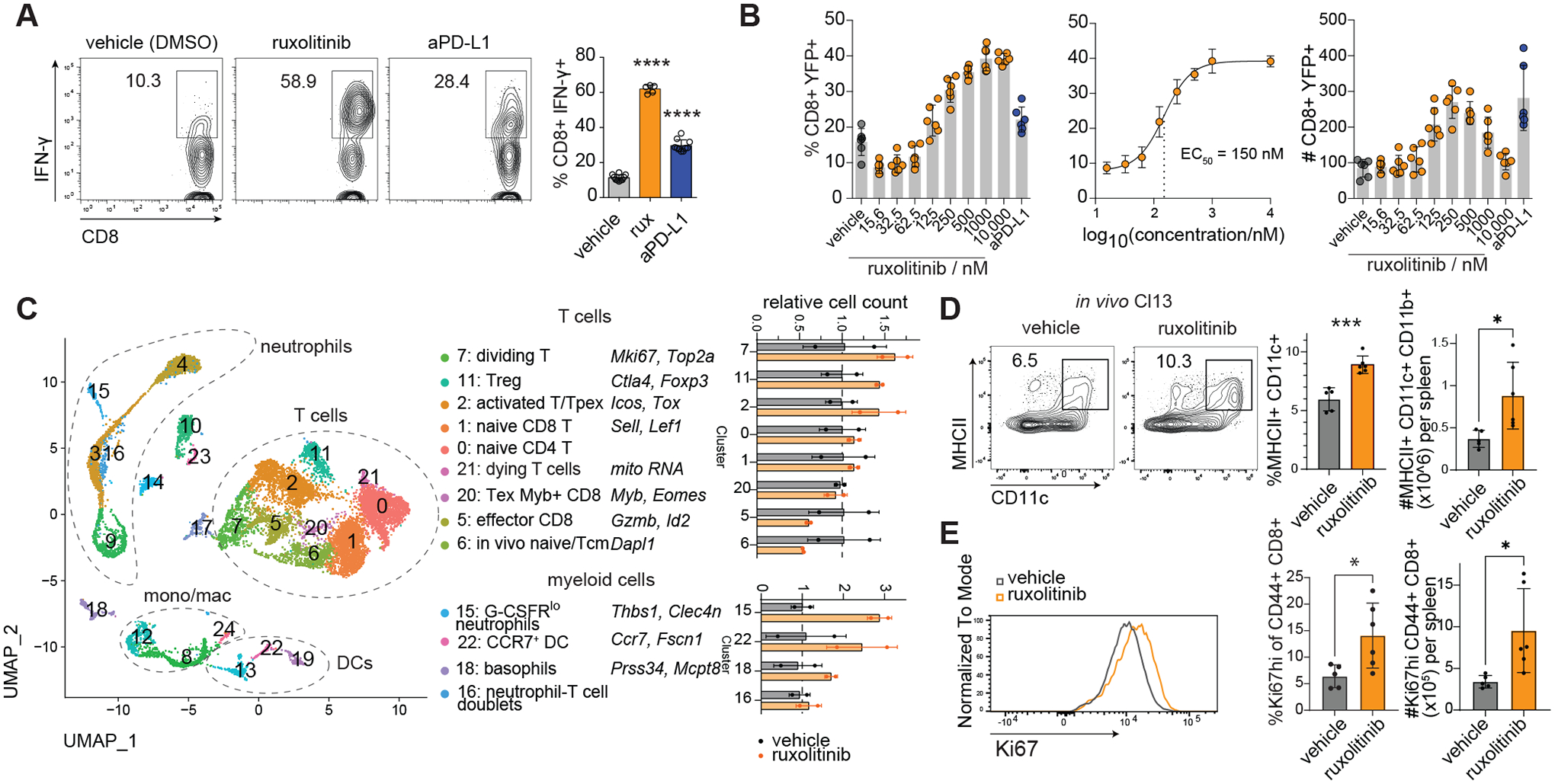
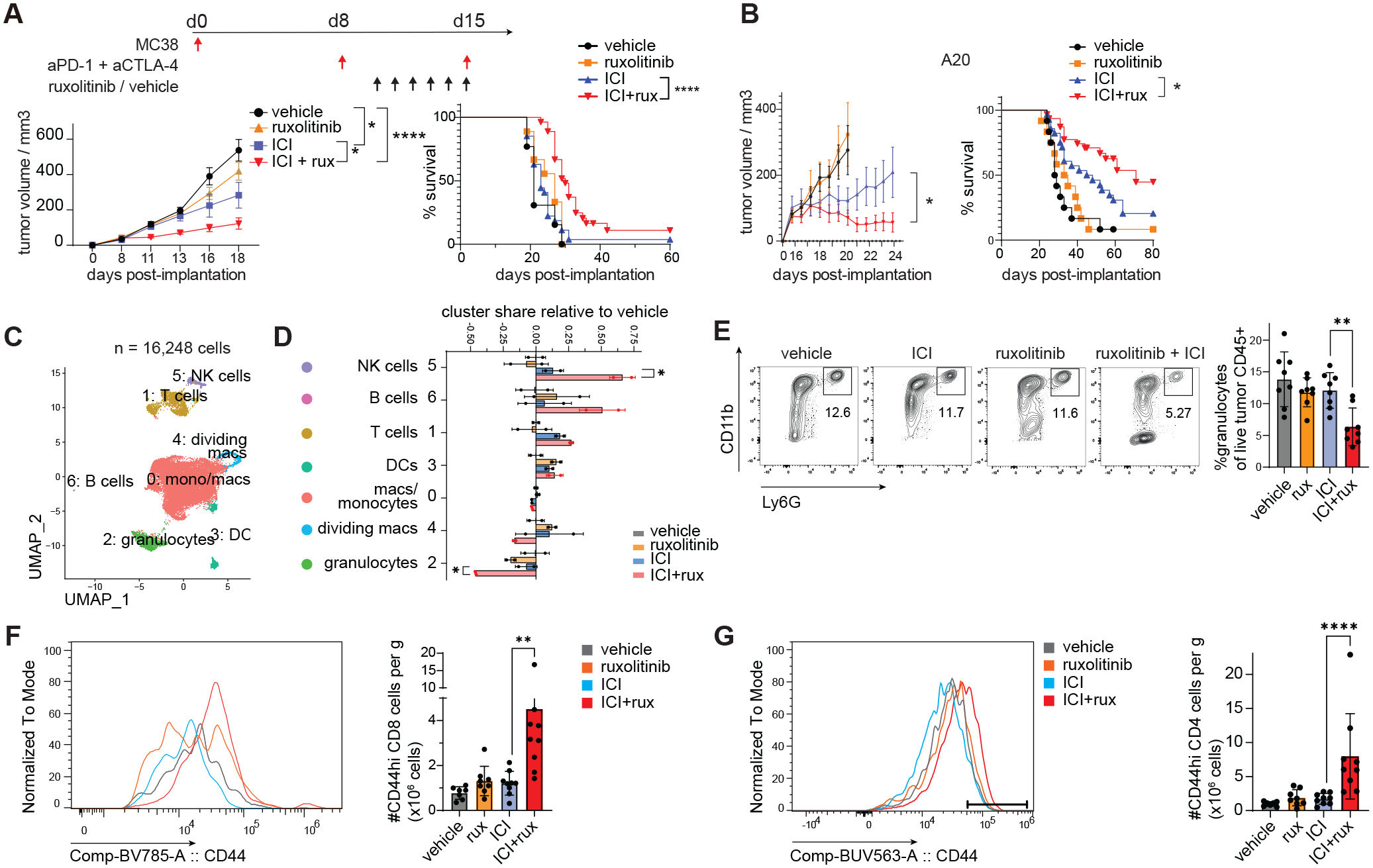
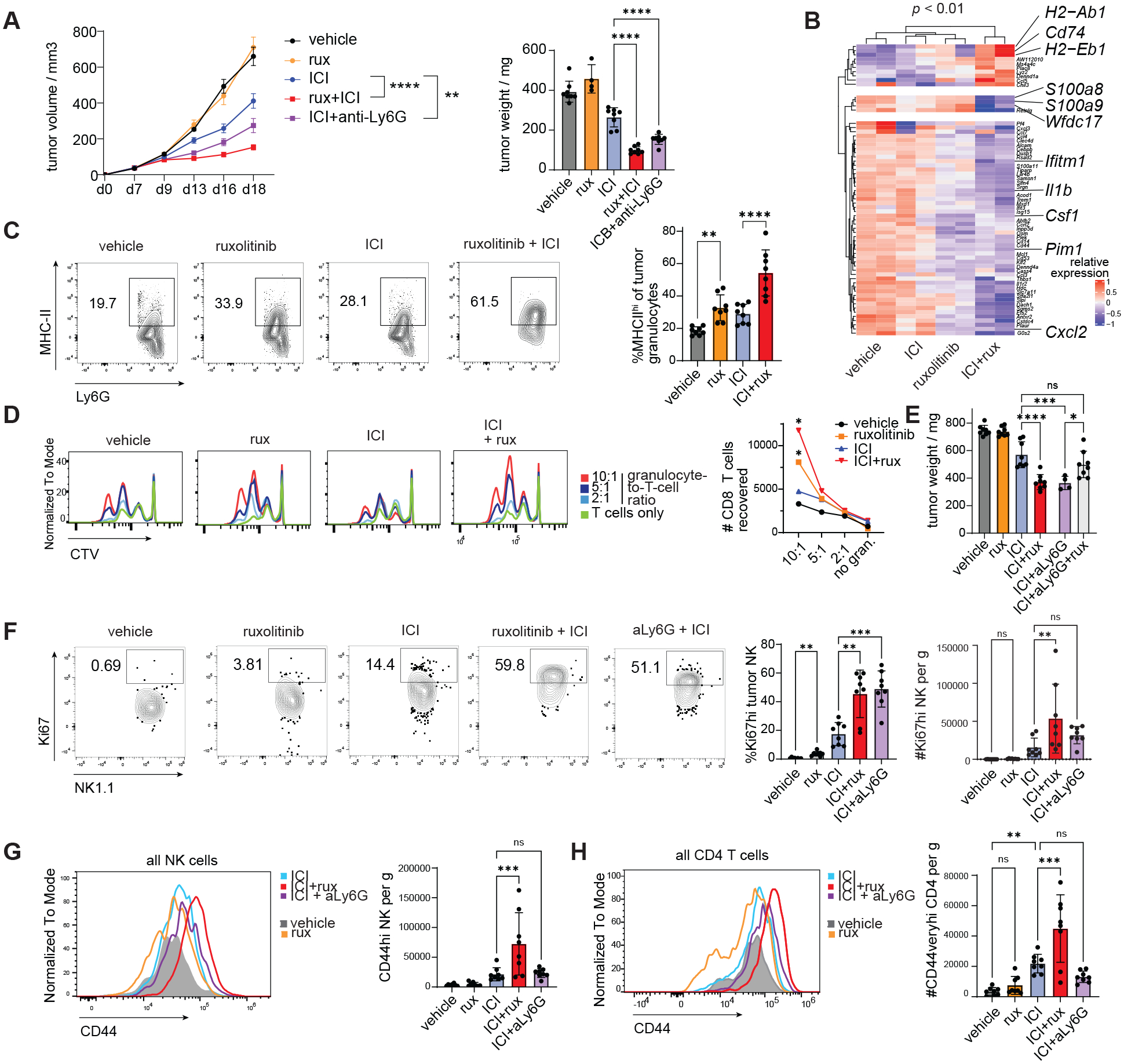
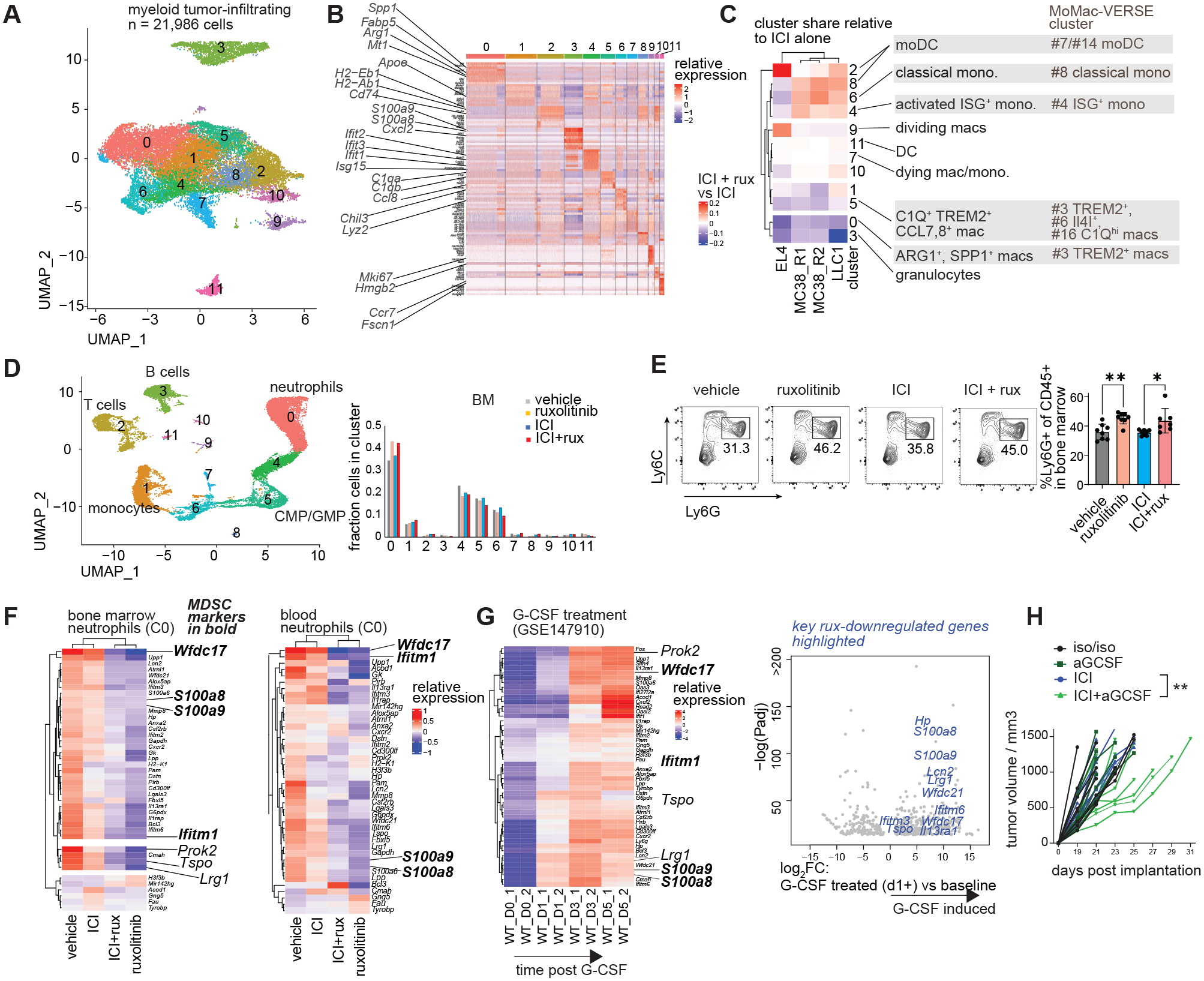
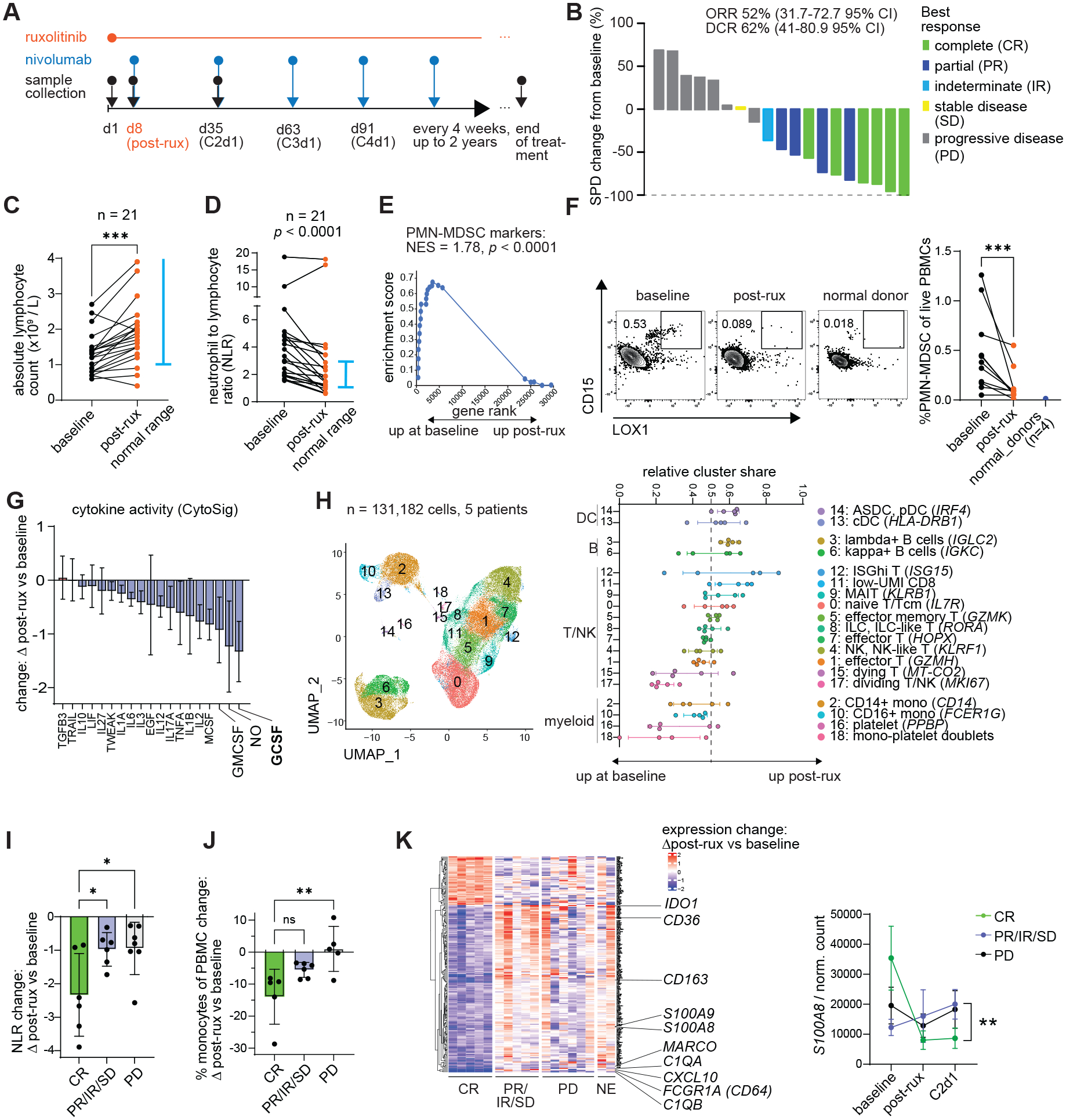
Unleashing antitumor T cell activity by checkpoint inhibitor immunotherapy is effective in cancer patients, but clinical responses are limited. Cytokine signaling through the Janus kinase (JAK)-signal transducer and activator of transcription (STAT) pathway correlates with checkpoint immunotherapy resistance. We report a phase I clinical trial of the JAK inhibitor ruxolitinib with anti-PD-1 antibody nivolumab in Hodgkin lymphoma patients relapsed or refractory following checkpoint inhibitor immunotherapy. The combination yielded a best overall response rate of 53% (10/19). Ruxolitinib significantly reduced neutrophil-to-lymphocyte ratios and percentages of myeloid suppressor cells but increased numbers of cytokine-producing T cells. Ruxolitinib rescued the function of exhausted T cells and enhanced the efficacy of immune checkpoint blockade in preclinical solid tumor and lymphoma models. This synergy was characterized by a switch from suppressive to immunostimulatory myeloid cells, which enhanced T cell division.
Conflict of interest statement
Figures
References
-
- Hotchkiss RS, Moldawer LL, Parallels between Cancer and Infectious Disease. New England Journal of Medicine 371, 380–383 (2014). - PubMed
-
- Barber DL, Wherry EJ, Masopust D, Zhu B, Allison JP, Sharpe AH, Freeman GJ, Ahmed R, Restoring function in exhausted CD8 T cells during chronic viral infection. Nature 439, 682–687 (2006). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
