

Machine learning predicts cerebral vasospasm in patients with subarachnoid haemorrhage
- PMID: 38901147
- PMCID: PMC11245940
- DOI: 10.1016/j.ebiom.2024.105206
Machine learning predicts cerebral vasospasm in patients with subarachnoid haemorrhage
Abstract
Background: Cerebral vasospasm (CV) is a feared complication which occurs after 20-40% of subarachnoid haemorrhage (SAH). It is standard practice to admit patients with SAH to intensive care for an extended period of resource-intensive monitoring. We used machine learning to predict CV requiring verapamil (CVRV) in the largest and only multi-center study to date.
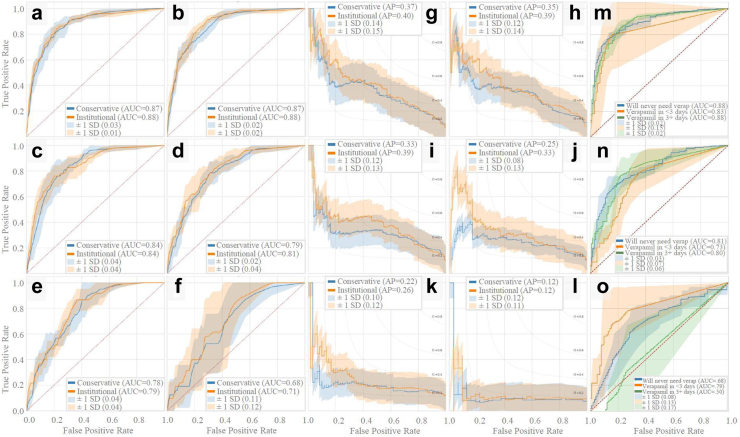
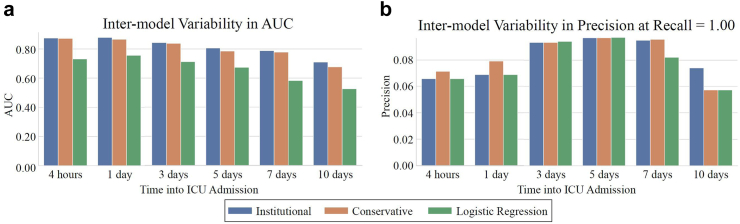
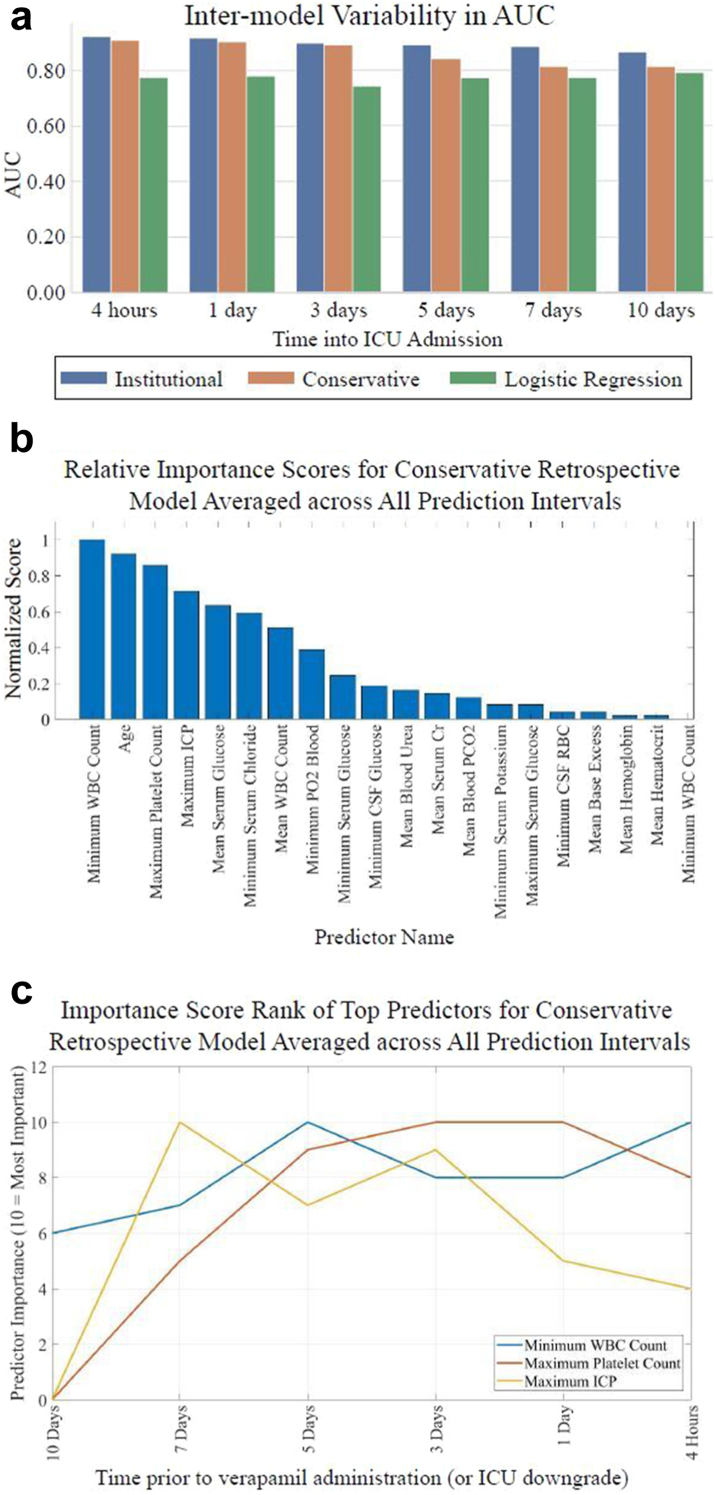
Methods: Patients with SAH admitted to UCLA from 2013 to 2022 and a validation cohort from VUMC from 2018 to 2023 were included. For each patient, 172 unique intensive care unit (ICU) variables were extracted through the primary endpoint, namely first verapamil administration or no verapamil. At each institution, a light gradient boosting machine (LightGBM) was trained using five-fold cross validation to predict the primary endpoint at various hospitalization timepoints.
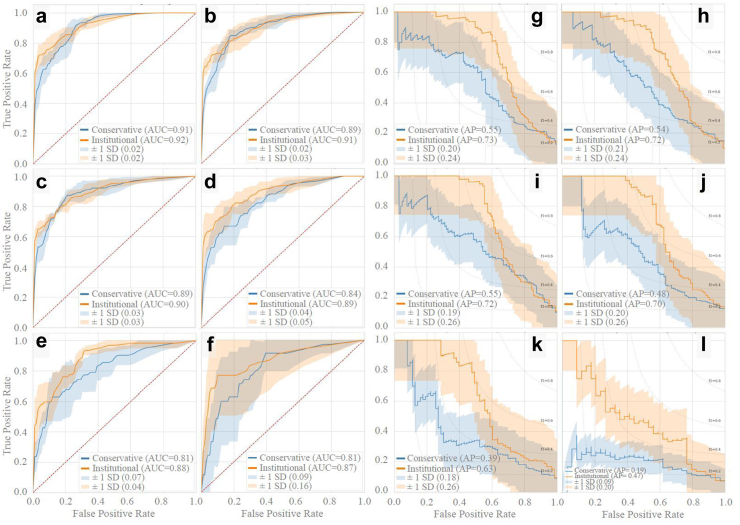
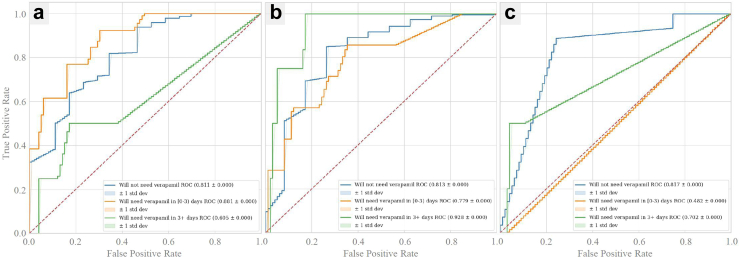
Findings: A total of 1750 patients were included from UCLA, 125 receiving verapamil. LightGBM achieved an area under the ROC (AUC) of 0.88 > 1 week in advance and ruled out 8% of non-verapamil patients with zero false negatives. Our models predicted "no CVRV" vs "CVRV within three days" vs "CVRV after three days" with AUCs = 0.88, 0.83, and 0.88, respectively. From VUMC, 1654 patients were included, 75 receiving verapamil. VUMC predictions averaged within 0.01 AUC points of UCLA predictions.
Interpretation: We present an accurate and early predictor of CVRV using machine learning with multi-center validation. This represents a significant step towards optimized clinical management and resource allocation in patients with SAH.
Funding: Robert E. Freundlich is supported by National Center for Advancing Translational Sciences federal grant UL1TR002243 and National Heart, Lung, and Blood Institute federal grant K23HL148640; these funders did not play any role in this study. The National Institutes of Health supports Vanderbilt University Medical Center which indirectly supported these research efforts. Neither this study nor any other authors personally received financial support for the research presented in this manuscript. No support from pharmaceutical companies was received.
Keywords: Cerebral vasospasm; Machine learning; Prediction; Verapamil.
Published by Elsevier B.V.
Conflict of interest statement
Declaration of interests The National Institutes of Health supports Vanderbilt University Medical Center, a participating institution in this study. Robert E. Freundlich is a consultant for Oak Hill Clinical Informatics, an expert witness for Hall Booth Smith, P.C., a Data and Safety Monitoring Board (DSMB) member for the Protocol and Statistical Analysis Plan for the Mode of Ventilation During Critical Illness (MODE) Trial, and the Treasurer for the Society of Technology in Anesthesia. Geoffrey Colby is a consultant for Medtronic, Stryker Neurovascular, and Rapid Medical. Eilon Gabel is a clinical trial consultant for Merck, Inc and unpaid co-founder of Extrico Health, Inc. All other authors have no conflict of interest. No author received financial support in conjunction with the generation of this submission.
Figures
Update of
-
Machine Learning Predicts Cerebral Vasospasm in Subarachnoid Hemorrhage Patients.Res Sq [Preprint]. 2024 Feb 5:rs.3.rs-3617246. doi: 10.21203/rs.3.rs-3617246/v1. Res Sq. 2024. Update in: EBioMedicine. 2024 Jul;105:105206. doi: 10.1016/j.ebiom.2024.105206. PMID: 38405758 Free PMC article. Updated. Preprint.
References
-
- Dorsch N.W.C., King M.T. A review of cerebral vasospasm in aneurysmal subarachnoid haemorrhage part I: incidence and effects. J Clin Neurosci. 1994;1(1):19–26. https://pubmed.ncbi.nlm.nih.gov/18638721/ [cited 2022 Nov 17]. Available from: - PubMed
-
- EEG monitoring to detect vasospasm after subarachnoid hemorrhage |…. https://www.reliasmedia.com/articles/34004-eeg-monitoring-to-detect-vaso... [cited 2022 Nov 17]. Available from:
-
- Frontera J.A., Fernandez A., Schmidt J.M., et al. Defining vasospasm after subarachnoid hemorrhage. Stroke. 2009;40(6):1963–1968. https://www.ahajournals.org/doi/abs/10.1161/STROKEAHA.108.544700 [cited 2022 Nov 17]. Available from: - DOI - PubMed
-
- Diringer M.N., Bleck T.P., Hemphill J.C., et al. Critical care management of patients following aneurysmal subarachnoid hemorrhage: recommendations from the Neurocritical care society's multidisciplinary consensus conference. Neurocrit Care. 2011;15(2):211–240. https://pubmed.ncbi.nlm.nih.gov/21773873/ [cited 2022 Nov 17]. Available from: - PubMed
