

Severe non-hepatic hyperammonaemic encephalopathy in an immunocompromised adolescent with enterocolitis
- PMID: 38901854
- PMCID: PMC11191012
- DOI: 10.1136/bcr-2023-256225
Severe non-hepatic hyperammonaemic encephalopathy in an immunocompromised adolescent with enterocolitis
Abstract
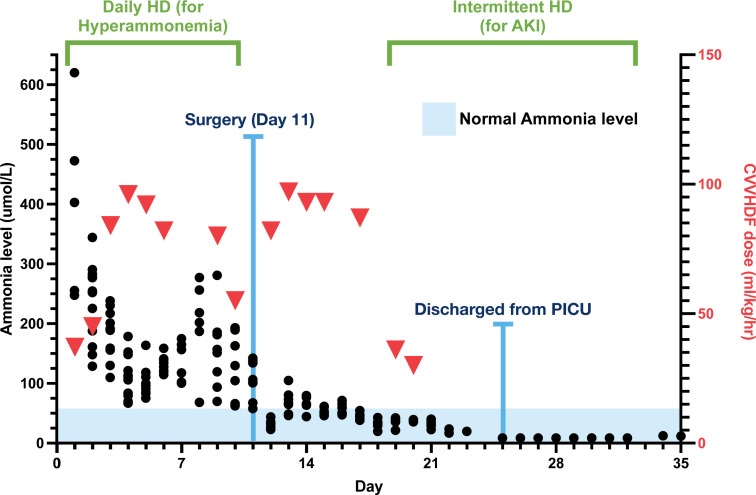
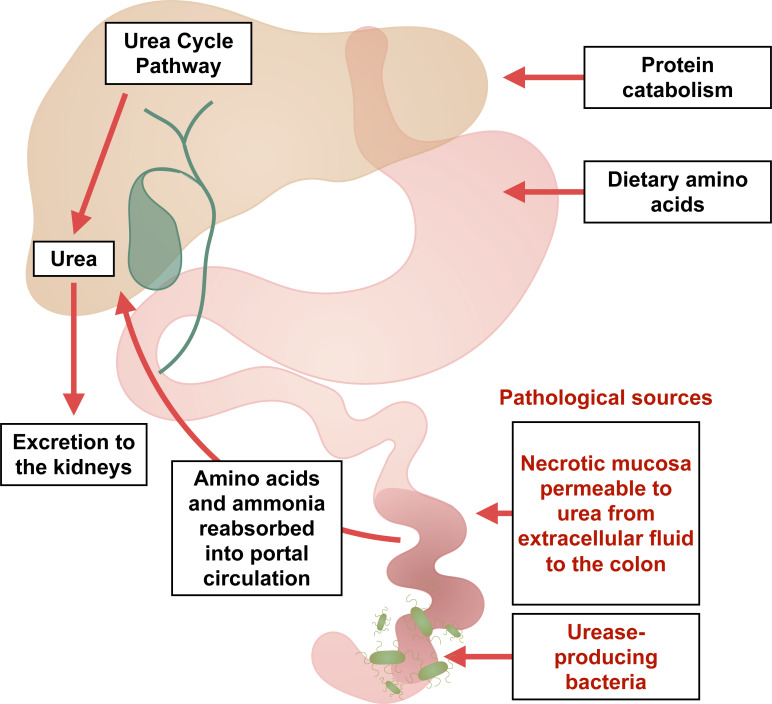
Non-hepatic causes of hyperammonaemia are uncommon relative to hepatic aetiologies. An adolescent female was admitted to the hospital with a diagnosis of very severe aplastic anaemia. During her treatment with immunosuppressive therapy, she developed neutropenic enterocolitis, pseudomonal bacteraemia and hyperammonaemia. A combination of intermittent haemodialysis and high-volume continuous veno-venous haemodiafiltration (CVVHDF) was required to manage the hyperammonaemia. Despite a thorough investigation, there were no hepatic, metabolic or genetic aetiologies identified that explained the hyperammonaemia. The hyperammonaemia resolved only after the surgical resection of her inflamed colon, following which she was successfully weaned off from the renal support. This is a novel case report of hyperammonaemia of non-hepatic origin secondary to widespread inflammation of the colon requiring surgical resection in an immunocompromised patient. This case also highlights the role of high-volume CVVHDF in augmenting haemodialysis in the management of severe refractory hyperammonaemia.
Keywords: Haematology (drugs and medicines); Haematology (incl blood transfusion); Hepatitis other; Infection (gastroenterology); Paediatric intensive care.
© BMJ Publishing Group Limited 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources