

Challenges and opportunities in cancer immunotherapy: a Society for Immunotherapy of Cancer (SITC) strategic vision
- PMID: 38901879
- PMCID: PMC11191773
- DOI: 10.1136/jitc-2024-009063
Challenges and opportunities in cancer immunotherapy: a Society for Immunotherapy of Cancer (SITC) strategic vision
Abstract
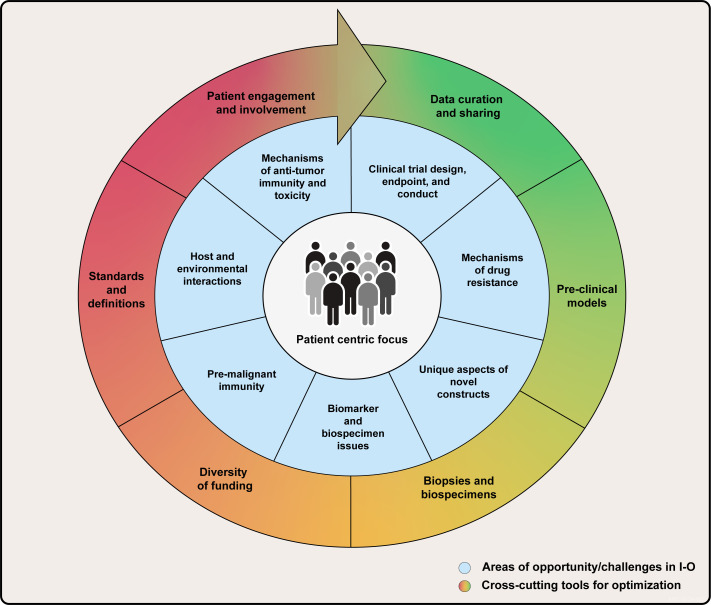
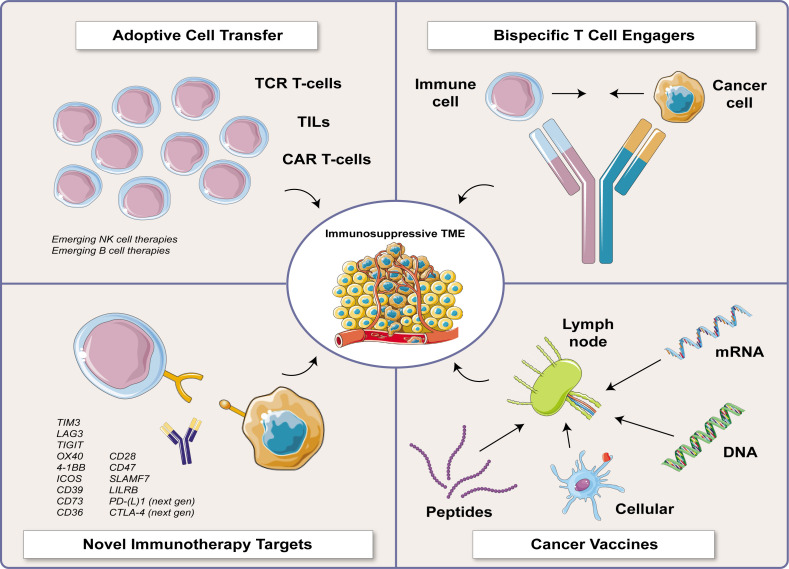
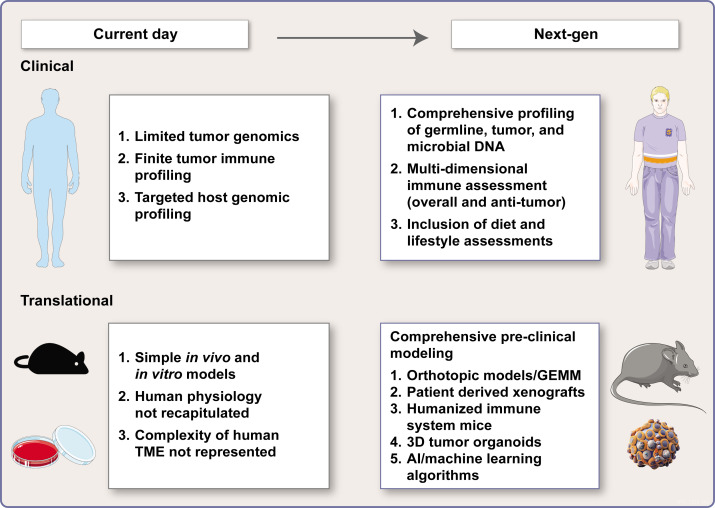
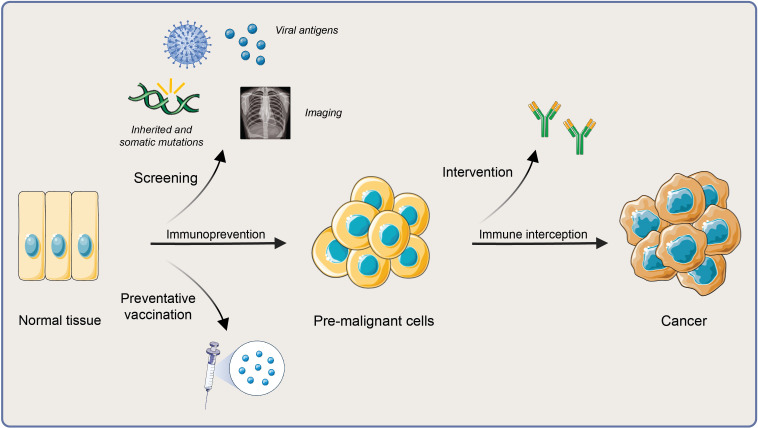
Cancer immunotherapy has flourished over the last 10-15 years, transforming the practice of oncology and providing long-term clinical benefit to some patients. During this time, three distinct classes of immune checkpoint inhibitors, chimeric antigen receptor-T cell therapies specific for two targets, and two distinct classes of bispecific T cell engagers, a vaccine, and an oncolytic virus have joined cytokines as a standard of cancer care. At the same time, scientific progress has delivered vast amounts of new knowledge. For example, advances in technologies such as single-cell sequencing and spatial transcriptomics have provided deep insights into the immunobiology of the tumor microenvironment. With this rapid clinical and scientific progress, the field of cancer immunotherapy is currently at a critical inflection point, with potential for exponential growth over the next decade. Recognizing this, the Society for Immunotherapy of Cancer convened a diverse group of experts in cancer immunotherapy representing academia, the pharmaceutical and biotechnology industries, patient advocacy, and the regulatory community to identify current opportunities and challenges with the goal of prioritizing areas with the highest potential for clinical impact. The consensus group identified seven high-priority areas of current opportunity for the field: mechanisms of antitumor activity and toxicity; mechanisms of drug resistance; biomarkers and biospecimens; unique aspects of novel therapeutics; host and environmental interactions; premalignant immunity, immune interception, and immunoprevention; and clinical trial design, endpoints, and conduct. Additionally, potential roadblocks to progress were discussed, and several topics were identified as cross-cutting tools for optimization, each with potential to impact multiple scientific priority areas. These cross-cutting tools include preclinical models, data curation and sharing, biopsies and biospecimens, diversification of funding sources, definitions and standards, and patient engagement. Finally, three key guiding principles were identified that will both optimize and maximize progress in the field. These include engaging the patient community; cultivating diversity, equity, inclusion, and accessibility; and leveraging the power of artificial intelligence to accelerate progress. Here, we present the outcomes of these discussions as a strategic vision to galvanize the field for the next decade of exponential progress in cancer immunotherapy.
Keywords: Education; Hematologic Malignancies; Immune modulatory; Immune related adverse event - irAE; Solid tumor.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: LAE, employee, Ankyra Therapeutics; researcher, AbbVie, AstraZeneca, Bolt Therapeutics, Bristol Meyers Squibb, Compugen, Corvus, CytomX, EMD Serono, Genentech, F Hoffman La Roche, Immune Onc, Merck, Next Cure, Silverback, Takeda, and Tempest; consultant/advisor/speaker, AstraZeneca, BioLineRx, DNAMx, Genentech, F Hoffman La Roche, GPCR, Gilead, Immune Onc, Immunitas, Immutep, Lilly, Macrogenics, Mersana, and Shionogi; royalty and patent beneficiary, potential for royalties in the future from Molecuvax; publicly traded stocks, potential for stock options in the future from Ankyra Therapeutics; Other, NSABP Foundation, Translational Breast Cancer Research Consortium, Breast Cancer Research Foundation, NCI, Department of Defense, Johns Hopkins University, University of California San Francisco, Cornell University, Dana-Farber Cancer Institute, and Stand Up to Cancer. These are grants from non-industry entities. TCB, advisory board, Kalivir, Tabby; consultant, Galvanize, Attivare, Mestag, and Tallac. CMC, consultant/advisor/speaker, Bayer, Elephas, Novartis, Nektar Therapeutics, and WiCell Research Institute. ACA, member of the SAB for Tizona Therapeutics, Trishula Therapeutics, Compass Therapeutics, Zumutor Biologics, Excepgen, and ImmuneOncia, which have interests in cancer immunotherapy. ACA is also a paid consultant for iTeos Therapeutics and Larkspur Biosciences. ACA is an inventor on patents related to the checkpoint receptor Tim-3. DC, executive role, ORIEN Patient Advisory Council. JLG, royalty and patent beneficiary, Bethesda Handbook of Clinical Oncology (royalty) and UpToDate (royalty); JITC interim editor-in-chief. PH, consultant/advisor/speaker, Dragonfly SAB and Immatics SAB. ADP, researcher, Astellas; consultant/advisor/speaker, ImmunoACT, Stromatis Pharma, GO Therapeutics, Astellas, and MaxCyte. PJR, employee, Novigenix and SA; researcher, Roche, pRED, Schilieren, and CH; consultant/advisor/speaker, Enterome, Transgene, and Maxivax. AWS, researcher, Biohaven Pharmaceuticals, Replimune, Morphogenesis, Shattuck Laboratories, Regeneron, and Merck; consultant/advisor/speaker, InStil Bio, Signatera, Merck, and Regeneron; royalty and patent beneficiary, UpToDate; and publicly traded stocks, Illumina. JAW reports compensation for speaker’s bureau and honoraria from PeerView and serves as a consultant and/or advisory board member for Gustave Roussy Cancer Center, EverImmune, OSE Immunotherapeutics, Bayer Therapeutics, James Cancer Center OSU, Daiichi Sanyko. SITC staff: EG, nothing to disclose. JW, nothing to disclose.
Figures
References
-
- Coley WB. The treatment of malignant tumors by repeated inoculations of erysipelas. with a report of ten original cases. 1893. Clin Orthop Relat Res 1991;3–11. - PubMed
-
- Rosenberg SA, Yang JC, Topalian SL, et al. . Treatment of 283 consecutive patients with metastatic melanoma or renal cell cancer using high-dose bolus interleukin 2. JAMA 1994;271:907–13. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical