

Volume control strategy and patient survival in sepsis-associated acute kidney injury receiving continuous renal replacement therapy: a randomized controlled trial with secondary analysis
- PMID: 38902283
- PMCID: PMC11190228
- DOI: 10.1038/s41598-024-64224-z
Volume control strategy and patient survival in sepsis-associated acute kidney injury receiving continuous renal replacement therapy: a randomized controlled trial with secondary analysis
Erratum in
-
Author Correction: Volume control strategy and patient survival in sepsis-associated acute kidney injury receiving continuous renal replacement therapy: a randomized controlled trial with secondary analysis.Sci Rep. 2024 Aug 22;14(1):19499. doi: 10.1038/s41598-024-70484-6. Sci Rep. 2024. PMID: 39174619 Free PMC article. No abstract available.
Abstract
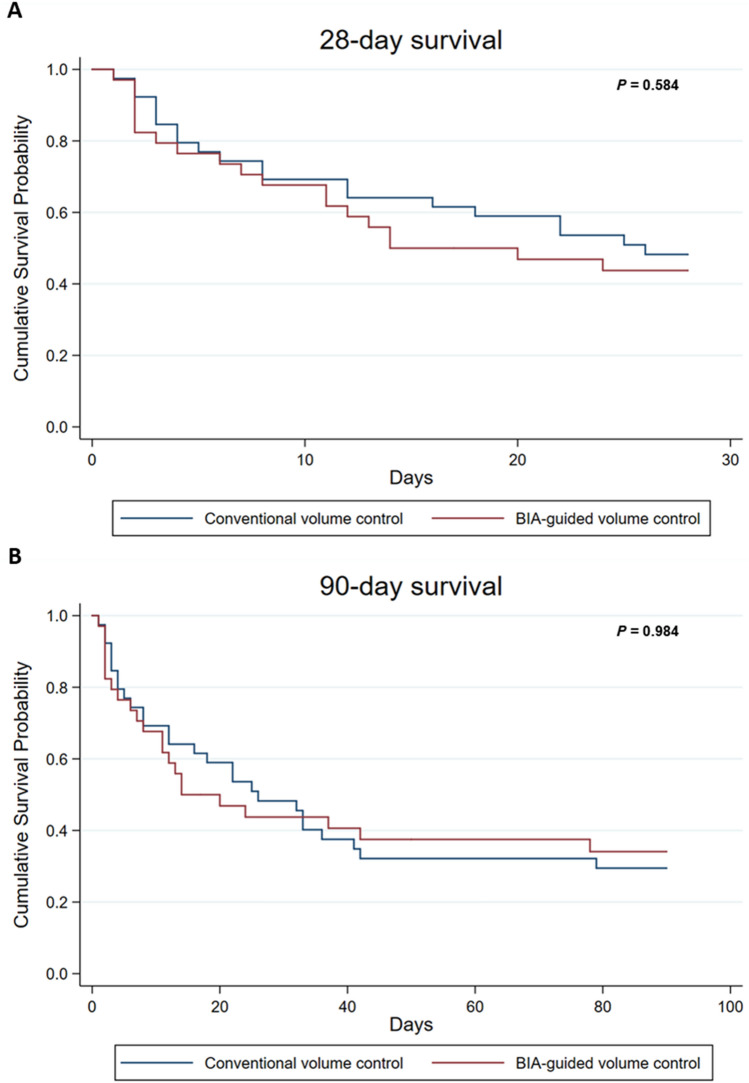
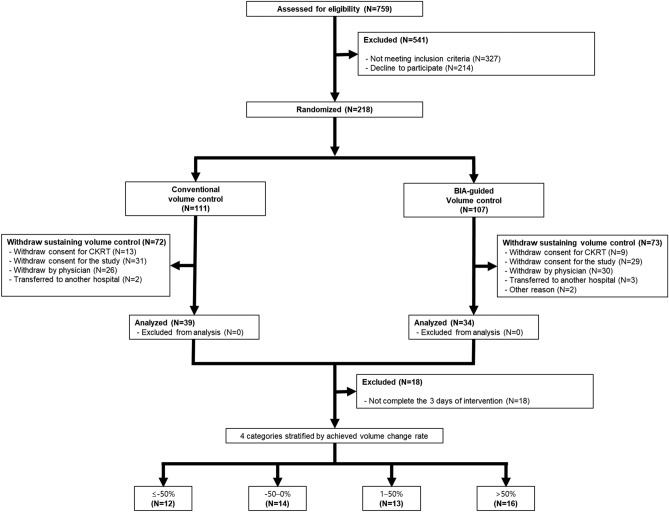
Optimal strategy for volume control and the clinical implication of achieved volume control are unknown in patients with sepsis-associated acute kidney injury (AKI) receiving continuous renal replacement therapy (CRRT). This randomized controlled trial aimed to compare the survival according to conventional or bioelectrical impedance analysis (BIA)-guided volume control strategy in patients with sepsis-associated AKI receiving CRRT. We also compared patient survival according to achieved volume accumulation rate ([cumulative fluid balance during 3 days × 100]/fluid overload measured by BIA at enrollment) as a post-hoc analysis. We randomly assigned patients to conventional volume control strategy (n = 39) or to BIA-guided volume control strategy (n = 34). There were no differences in 28-day mortality (HR, 1.19; 95% CI, 0.63-2.23) or 90-day mortality (HR, 0.99; 95% CI 0.57-1.75) between conventional and BIA-guided volume control group. In the secondary analysis, achieved volume accumulation rate was significantly associated with patient survival. Compared with the achieved volume accumulation rate of ≤ - 50%, the HRs (95% CIs) for the risk of 90-day mortality were 1.21 (0.29-5.01), 0.55 (0.12-2.48), and 7.18 (1.58-32.51) in that of - 50-0%, 1-50%, and > 50%, respectively. Hence, BIA-guided volume control in patients with sepsis-associated AKI receiving CRRT did not improve patient outcomes. In the secondary analysis, achieved volume accumulation rate was associated with patient survival.
Keywords: Bioelectrical impedance analysis; Continuous renal replacement therapy; Sepsis-associated acute kidney injury; Volume control.
© 2024. The Author(s).
Conflict of interest statement
Tae-Hyun Yoo reports research funding: Fresenius Medical Care, Korea. The other authors declared no competing interests. The opinions, results, and conclusions are those of the authors and are independent from this funding and data sources.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
