

Healthcare utilisation in people with long COVID: an OpenSAFELY cohort study
- PMID: 38902726
- PMCID: PMC11188519
- DOI: 10.1186/s12916-024-03477-x
Healthcare utilisation in people with long COVID: an OpenSAFELY cohort study
Abstract
Background: Long COVID potentially increases healthcare utilisation and costs. However, its impact on the NHS remains to be determined.
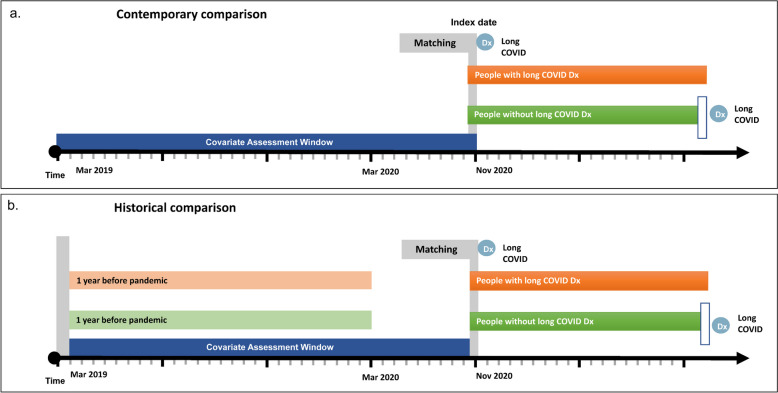
Methods: This study aims to assess the healthcare utilisation of individuals with long COVID. With the approval of NHS England, we conducted a matched cohort study using primary and secondary care data via OpenSAFELY, a platform for analysing anonymous electronic health records. The long COVID exposure group, defined by diagnostic codes, was matched with five comparators without long COVID between Nov 2020 and Jan 2023. We compared their total healthcare utilisation from GP consultations, prescriptions, hospital admissions, A&E visits, and outpatient appointments. Healthcare utilisation and costs were evaluated using a two-part model adjusting for covariates. Using a difference-in-difference model, we also compared healthcare utilisation after long COVID with pre-pandemic records.
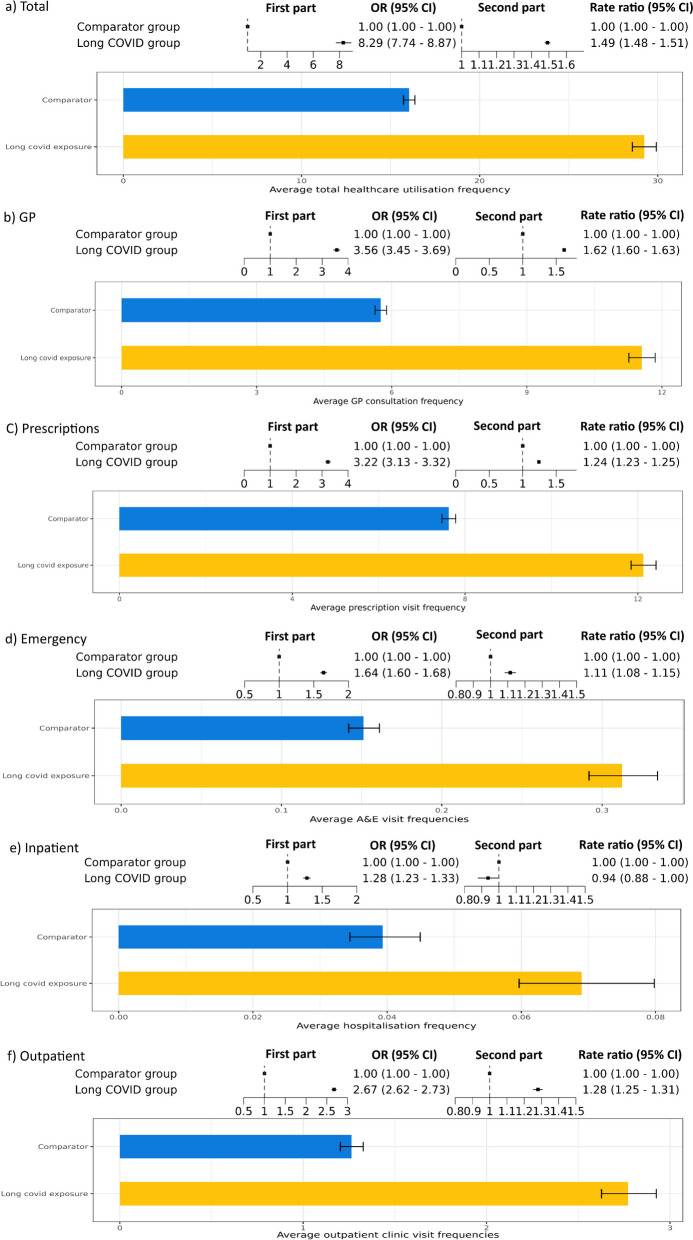
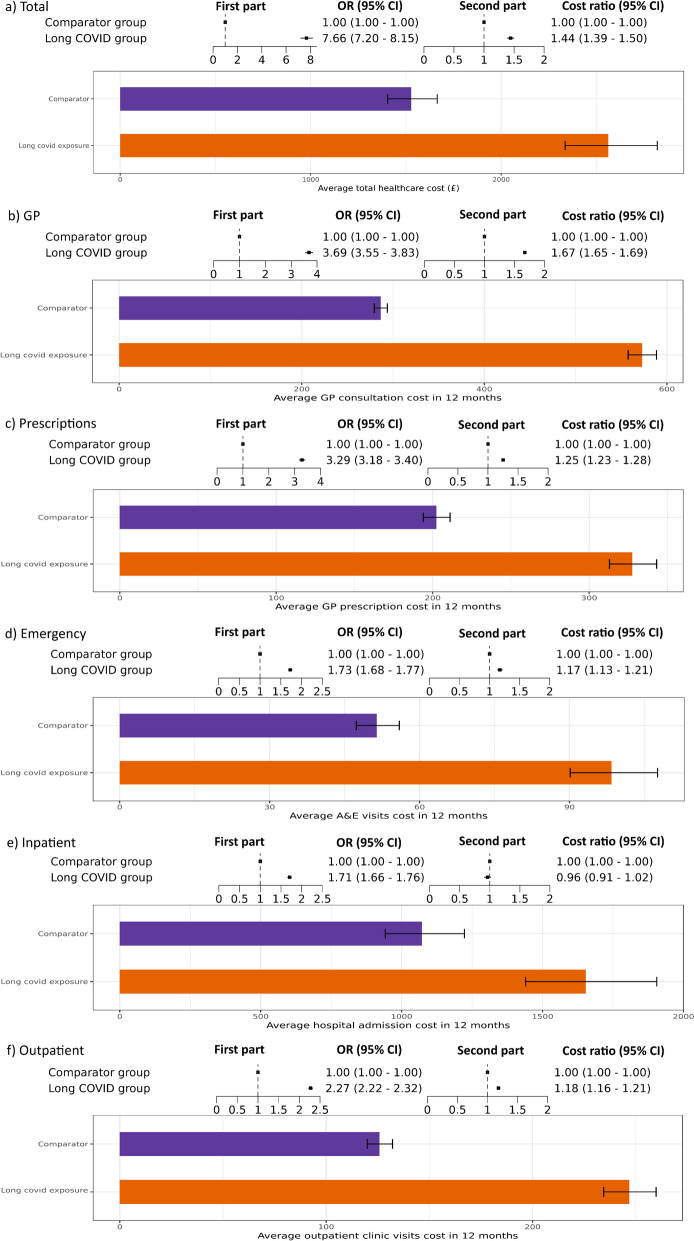
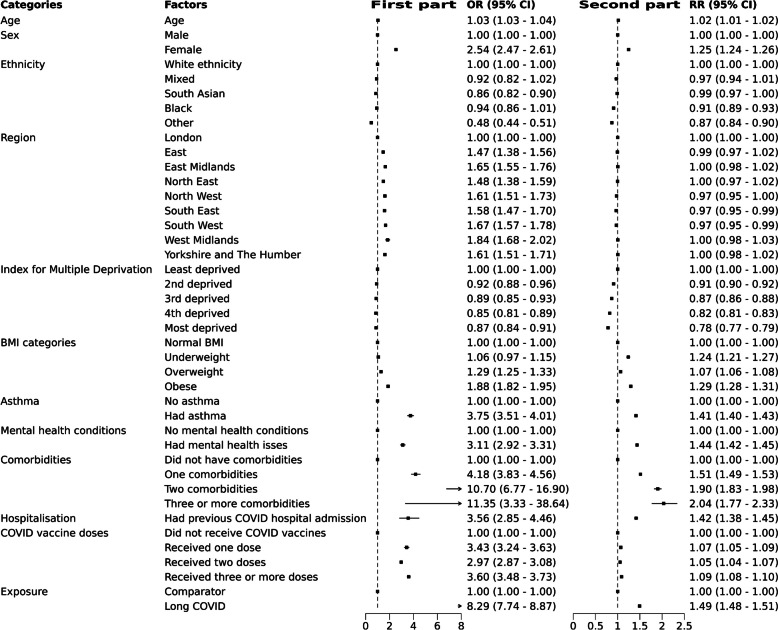
Results: We identified 52,988 individuals with a long COVID diagnosis, matched to 264,867 comparators without a diagnosis. In the 12 months post-diagnosis, there was strong evidence that those with long COVID were more likely to use healthcare resources (OR: 8.29, 95% CI: 7.74-8.87), and have 49% more healthcare utilisation (RR: 1.49, 95% CI: 1.48-1.51). Our model estimated that the long COVID group had 30 healthcare visits per year (predicted mean: 29.23, 95% CI: 28.58-29.92), compared to 16 in the comparator group (predicted mean visits: 16.04, 95% CI: 15.73-16.36). Individuals with long COVID were more likely to have non-zero healthcare expenditures (OR = 7.66, 95% CI = 7.20-8.15), with costs being 44% higher than the comparator group (cost ratio = 1.44, 95% CI: 1.39-1.50). The long COVID group costs approximately £2500 per person per year (predicted mean cost: £2562.50, 95% CI: £2335.60-£2819.22), and the comparator group costs £1500 (predicted mean cost: £1527.43, 95% CI: £1404.33-1664.45). Historically, individuals with long COVID utilised healthcare resources more frequently, but their average healthcare utilisation increased more after being diagnosed with long COVID, compared to the comparator group.
Conclusions: Long COVID increases healthcare utilisation and costs. Public health policies should allocate more resources towards preventing, treating, and supporting individuals with long COVID.
Keywords: Electronic health records; Facilities and services utilization; Health care costs; Long COVID.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests. BG is a Non-Executive Director at NHS Digital; he also receives personal income from speaking and writing for lay audiences on the misuse of science.
Figures

References
-
- NICE. COVID-19 rapid guideline: managing the long-term effects of COVID-19. 2023. - PubMed
-
- Office for National Statistics. Prevalence of ongoing symptoms following coronavirus (COVID-19) infection in the UK: 30 March 2023. 2023.
-
- Carlile O, Briggs A, Henderson AD, Butler-Cole BFC, Tazare J, Tomlinson LA, et al. Impact of long COVID on health-related quality-of-life: an OpenSAFELY population cohort study using patient-reported outcome measures (OpenPROMPT) The Lancet Reg Health - Eur. 2024;40:100908. doi: 10.1016/j.lanepe.2024.100908. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
