

Effect of prophylactic corticosteroids on postoperative neurocognitive dysfunction in the adult population: An updated systematic review, meta-analysis, and trial sequential analysis of randomised controlled trials
- PMID: 38903252
- PMCID: PMC11186528
- DOI: 10.4103/ija.ija_149_24
Effect of prophylactic corticosteroids on postoperative neurocognitive dysfunction in the adult population: An updated systematic review, meta-analysis, and trial sequential analysis of randomised controlled trials
Abstract
Background and aims: Postoperative neurocognitive dysfunction (PNCD) commonly occurs after surgery and prolongs hospital stays. Both direct noxious stimuli to the central nervous system and systemic inflammation have been implicated. Due to their potent anti-inflammatory effects, corticosteroids have been utilised to attenuate the incidence and severity of PNCD. This systematic review and meta-analysis strived to evaluate the prophylactic role of perioperative corticosteroids for PNCD.
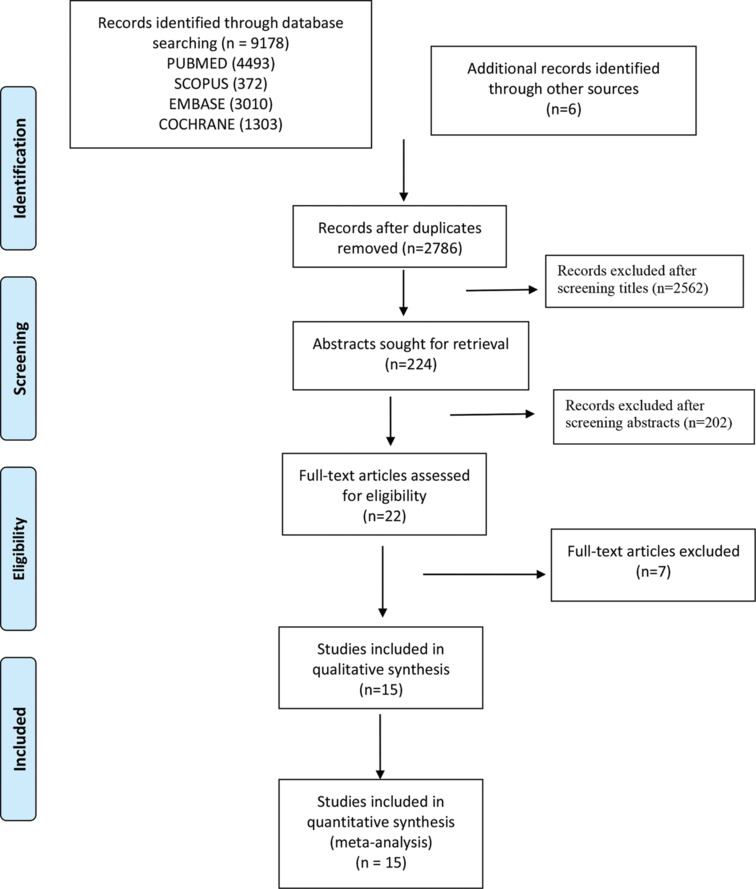
Methods: A search was run in pre-defined databases for randomised controlled trials (RCTs) assessing the role of corticosteroids in preventing PNCD. The incidence of PNCD within 1 month was the primary outcome. Secondary outcomes included the use of antipsychotic medications for the treatment, postoperative infection, and hospital length of stay. The results are exhibited as odds ratio (OR) and the mean difference (MD) with 95% confidence interval (CI).
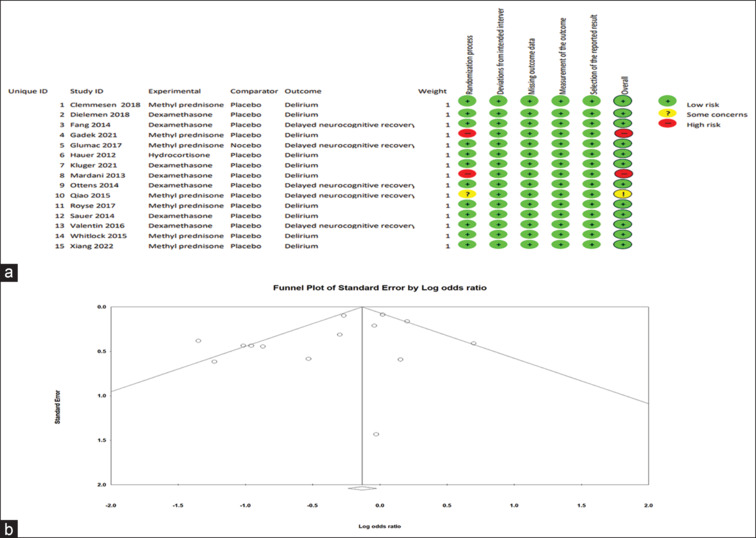
Results: Fifteen RCTs comprising 15,398 patients were included. The incidence of PNCD was significantly lower in the corticosteroid group than in the control group, with a pooled OR of 0.75 (95% CI 0.58, 0.96; P = 0.02; I2 = 66%). Trial sequential analysis showed the clinical benefit of corticosteroids in preventing PNCD; however, the requisite information size is still inadequate. The sub-group analysis supported the prophylactic effect of corticosteroids on delirium prevention but not on delayed neurocognitive recovery.
Conclusions: Our meta-analysis revealed statistically significant protective effects of corticosteroids on the incidence of PNCD. However, further studies are still needed to confirm the protective role of this commonly used and relatively safe strategy for preventing PNCD.
Keywords: Corticosteroids; delayed neurocognitive recovery; delirium; dexamethasone; meta-analysis; post-operative neurocognitive dysfunction; postoperative cognitive dysfunction; systematic review; trial sequential analysis.
Copyright: © 2024 Indian Journal of Anaesthesia.
Conflict of interest statement
There are no conflicts of interest.
Figures


Comment in
-
Effect of prophylactic corticosteroids on postoperative neurocognitive dysfunction.Indian J Anaesth. 2024 Sep;68(9):842. doi: 10.4103/ija.ija_709_24. Epub 2024 Aug 16. Indian J Anaesth. 2024. PMID: 39386392 Free PMC article. No abstract available.
-
Trial sequential analysis: Quality improvement for meta-analysis.Indian J Anaesth. 2024 Dec;68(12):1092-1094. doi: 10.4103/ija.ija_1051_24. Epub 2024 Dec 3. Indian J Anaesth. 2024. PMID: 39944024 Free PMC article. No abstract available.
References
-
- American Geriatrics Society expert panel on postoperative delirium in older adults Postoperative delirium in older adults: Best practice statement from the American Geriatrics Society. J Am Coll Surg. 2015;220:136–48.e1. - PubMed
-
- Evered L, Silbert B, Knopman DS, Scott DA, DeKosky ST, Rasmussen LS, et al. Recommendations for the nomenclature of cognitive change associated with anesthesia and surgery-2018. Anesth Analg. 2018;127:1189–95. - PubMed
-
- Bramley P, McArthur K, Blayney A, McCullagh I. Risk factors for postoperative delirium: An umbrella review of systematic reviews. Int J Surg. 2021;93:106063. doi: 10.1016/j.ijsu. 2021.106063. - PubMed
LinkOut - more resources
Full Text Sources