

Lung transplantation following controlled hypothermic storage with a portable lung preservation device: first multicenter European experience
- PMID: 38903974
- PMCID: PMC11187339
- DOI: 10.3389/fcvm.2024.1370543
Lung transplantation following controlled hypothermic storage with a portable lung preservation device: first multicenter European experience
Abstract
Introduction: Compared with traditional static ice storage, controlled hypothermic storage (CHS) at 4-10°C may attenuate cold-induced lung injury between procurement and implantation. In this study, we describe the first European lung transplant (LTx) experience with a portable CHS device.
Methods: A prospective observational study was conducted of all consecutively performed LTx following CHS (11 November 2022 and 31 January 2024) at two European high-volume centers. The LUNGguard device was used for CHS. The preservation details, total ischemic time, and early postoperative outcomes are described. The data are presented as median (range: minimum-maximum) values.
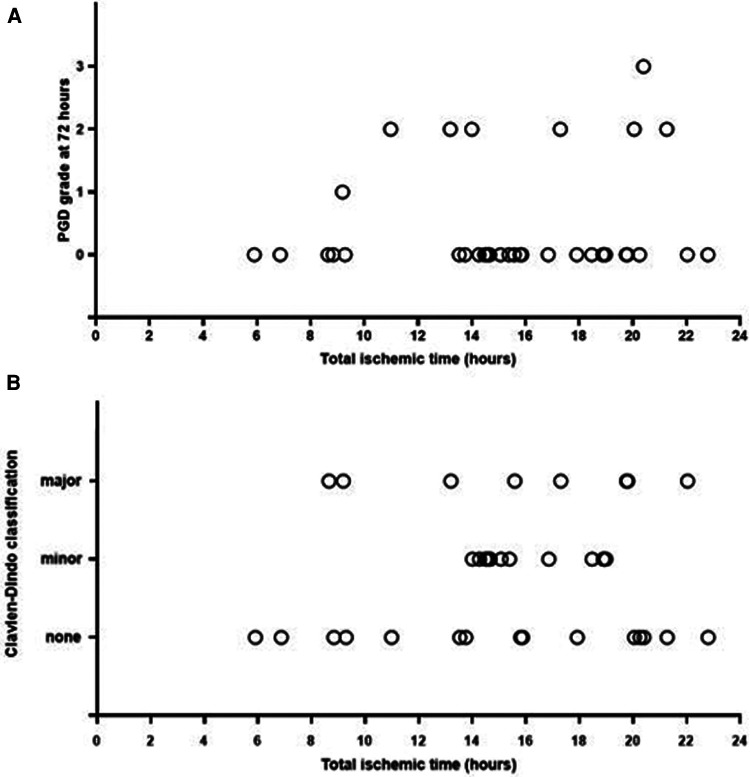
Results: A total of 36 patients underwent LTx (i.e., 33 bilateral, 2 single LTx, and 1 lobar). The median age was 61 (15-68) years; 58% of the patients were male; 28% of the transplantations had high-urgency status; and 22% were indicated as donation after circulatory death. In 47% of the patients, extracorporeal membrane oxygenation (ECMO) was used for perioperative support. The indications for using the CHS device were overnight bridging (n = 26), remote procurement (n = 4), rescue allocation (n = 2), logistics (n = 2), feasibility (n = 1), and extended-criteria donor (n = 1). The CHS temperature was 6.5°C (3.7°C-9.3°C). The preservation times were 11 h 18 (2 h 42-17 h 9) and 13 h 40 (4 h 5-19 h 36) for the first and second implanted lungs, respectively, whereas the total ischemic times were 13 h 38 (4 h 51-19 h 44) and 15 h 41 (5 h 54-22 h 48), respectively. The primary graft dysfunction grade 3 (PGD3) incidence rates were 33.3% within 72 h and 2.8% at 72 h. Intensive care unit stay was 8 (4-62) days, and the hospital stay was 28 (13-87) days. At the last follow-up [139 (7-446) days], three patients were still hospitalized. One patient died on postoperative day 7 due to ECMO failure. In-hospital Clavien-Dindo complications of 3b were observed in six (17%) patients, and 4a in seven (19%).
Conclusion: CHS seems safe and feasible despite the high-risk recipient and donor profiles, as well as extended preservation times. PGD3 at 72 h was observed in 2.8% of the patients. This technology could postpone LTx to daytime working hours. Larger cohorts and longer-term outcomes are required to confirm these observations.
Keywords: controlled hypothermic storage; lung preservation; overnight bridging; preservation temperature; preservation time; primary graft dysfunction; total ischemic time.
© 2024 Provoost, Novysedlak, Van Raemdonck, Van Slambrouck, Prisciandaro, Vandervelde, Barbarossa, Jin, Denaux, De Leyn, Van Veer, Depypere, Jansen, Pirenne, Neyrinck, Bouneb, Ingels, Jacobs, Godinas, De Sadeleer, Vos, Svorcova, Vajter, Kolarik, Tavandzis, Havlin, Ozaniak Strizova, Pozniak, Simonek, Vachtenheim Jr, Lischke and Ceulemans.
Conflict of interest statement
In relation to this manuscript, we disclose that Paragonix granted five LUNGguard™ devices to the authors to test their feasibility. No financial compensation was granted. DVR is supported by the Broere Charitable Foundation. RV is a senior Clinical Research Fellow of the Research Foundation-Flanders (FWO) (#1803521N). LJC is a senior Clinical Research Fellow of the Research Foundation-Flanders (FWO) (#18E2B24N). LJC is supported by a KU Leuven University Chair funded by Medtronic. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources