

Loss of microRNA-15a/16-1 function promotes neuropathological and functional recovery in experimental traumatic brain injury
- PMID: 38912585
- PMCID: PMC11383186
- DOI: 10.1172/jci.insight.178650
Loss of microRNA-15a/16-1 function promotes neuropathological and functional recovery in experimental traumatic brain injury
Abstract
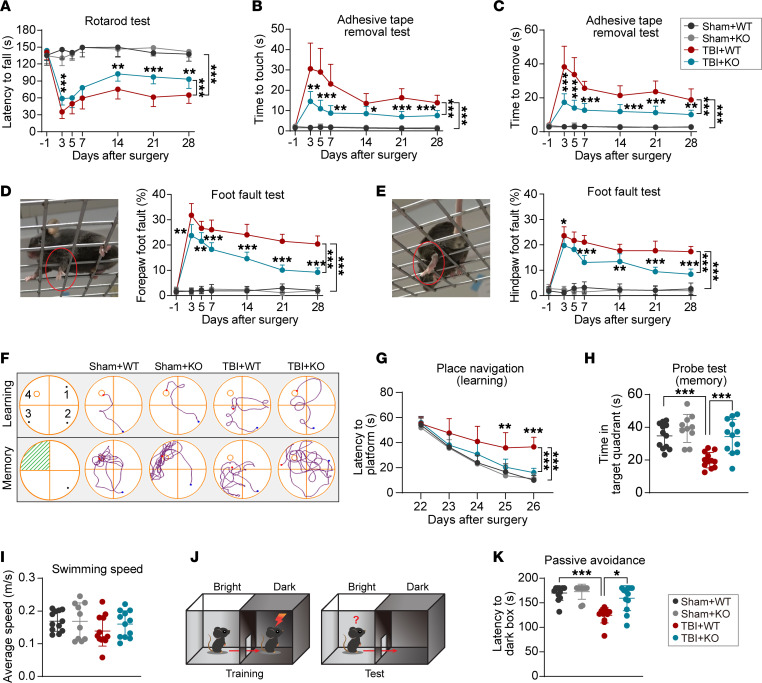
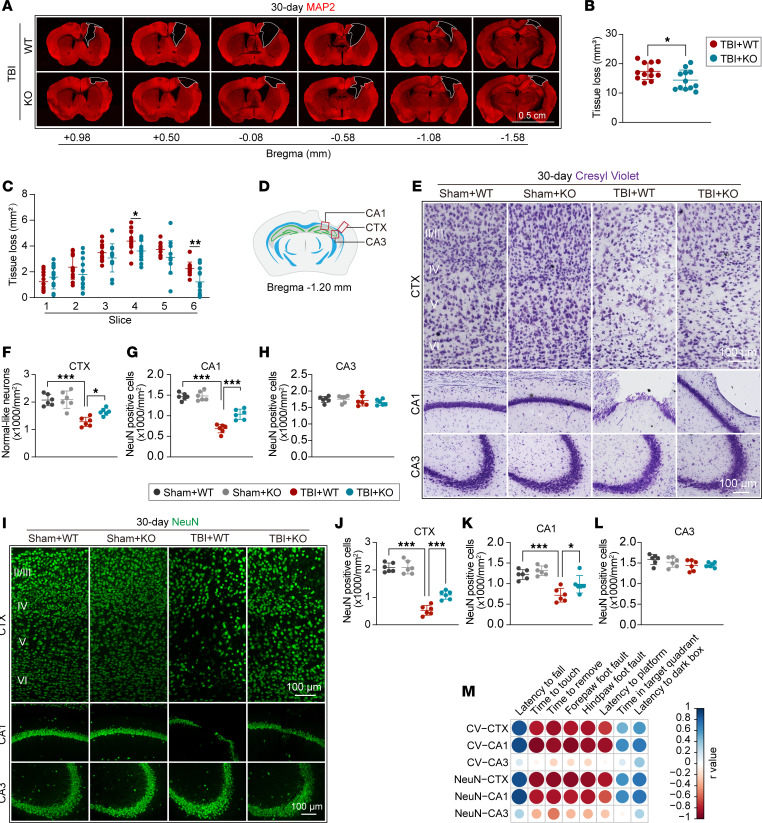
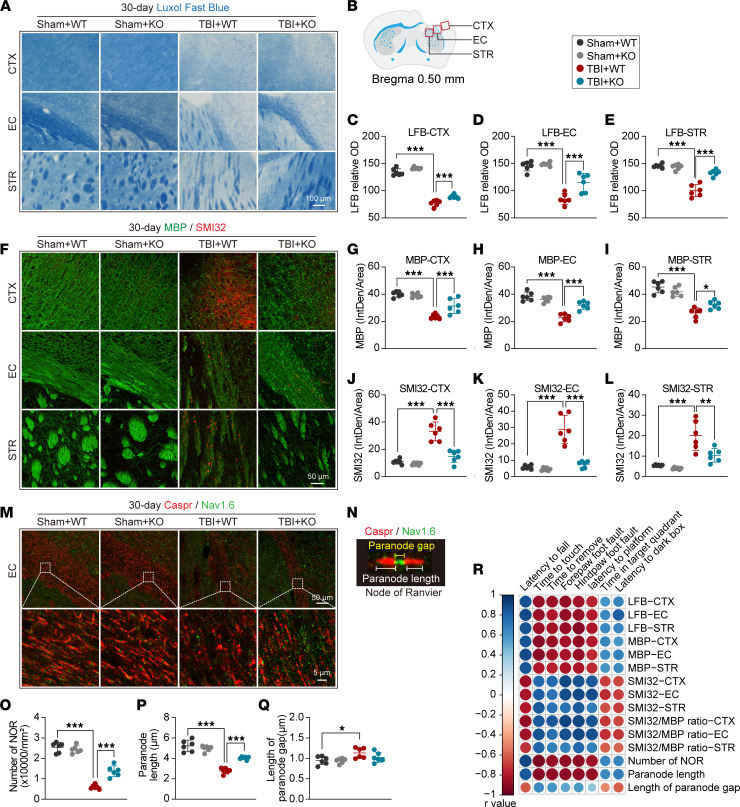
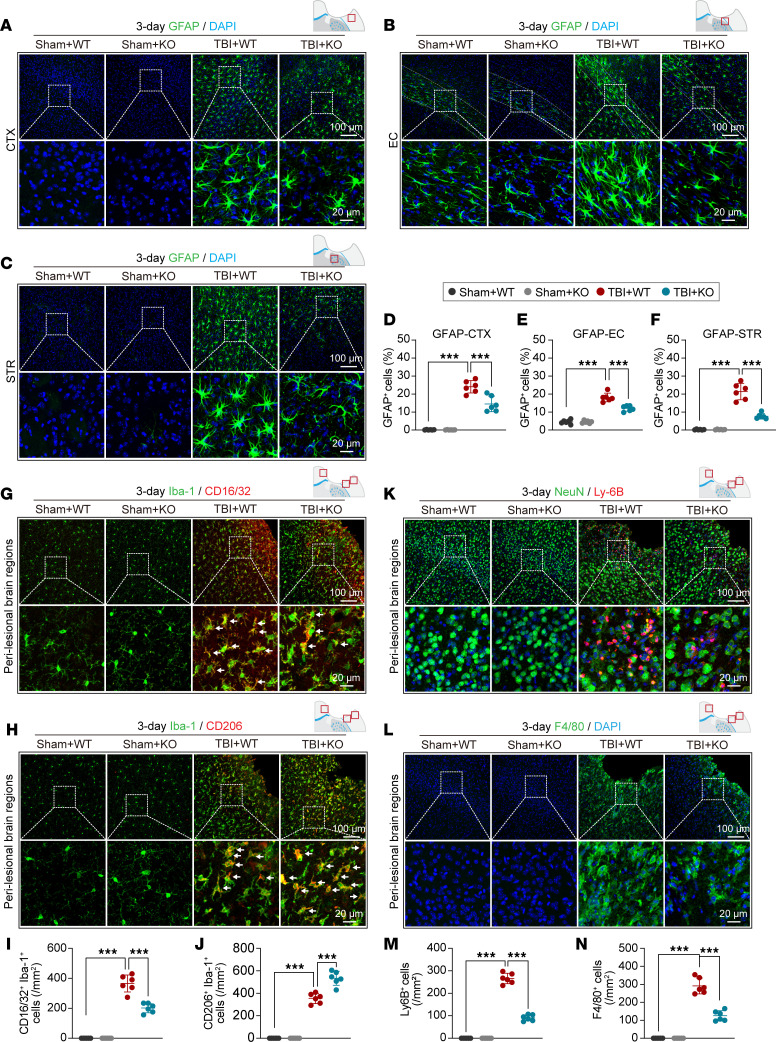
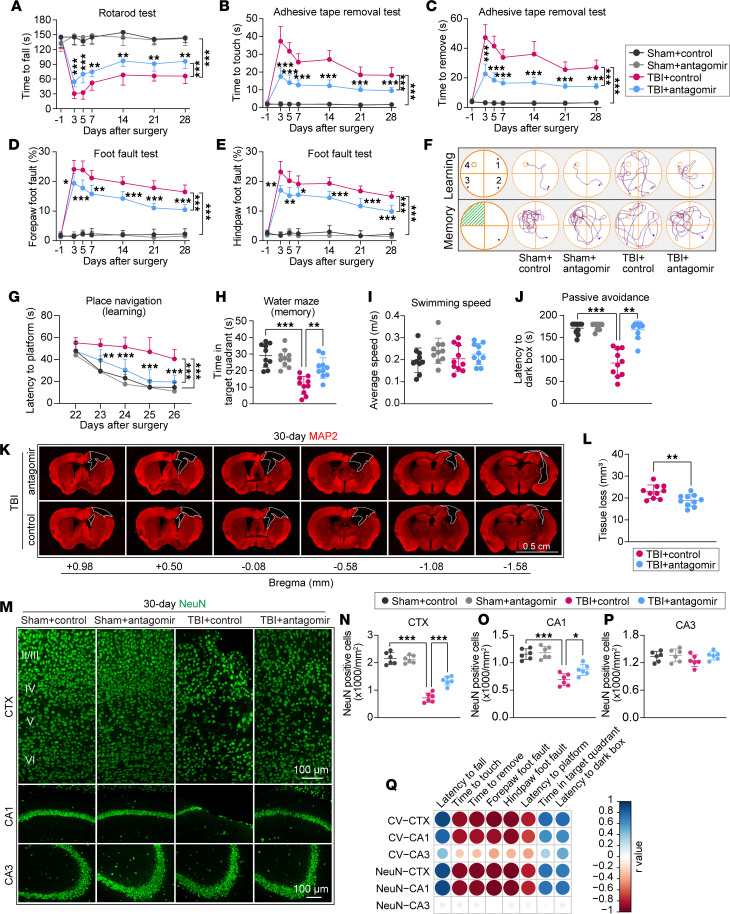
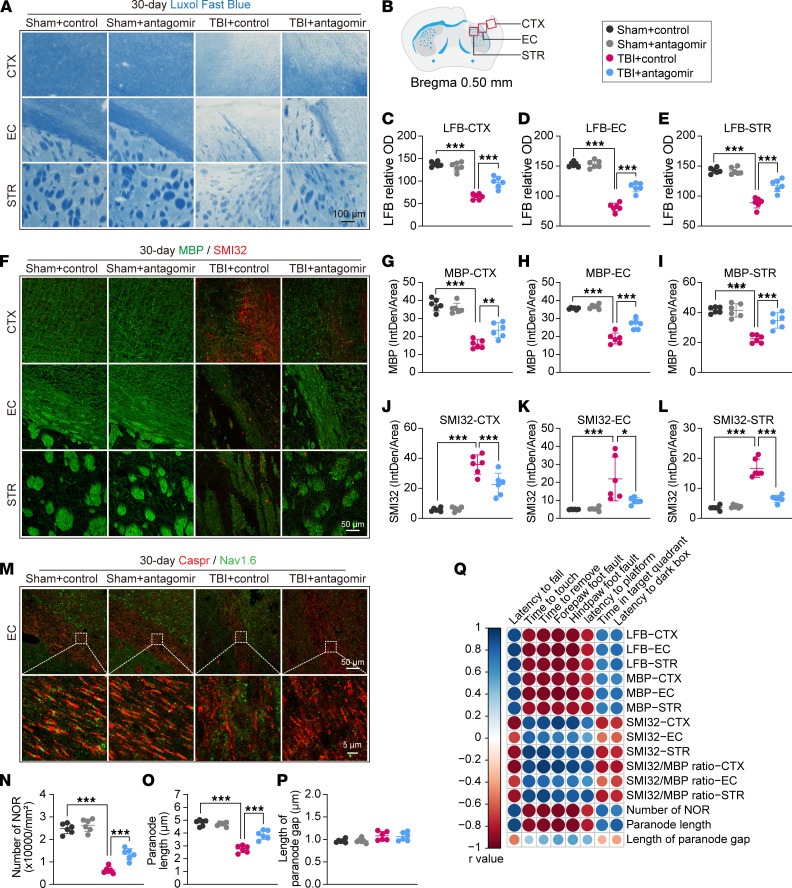
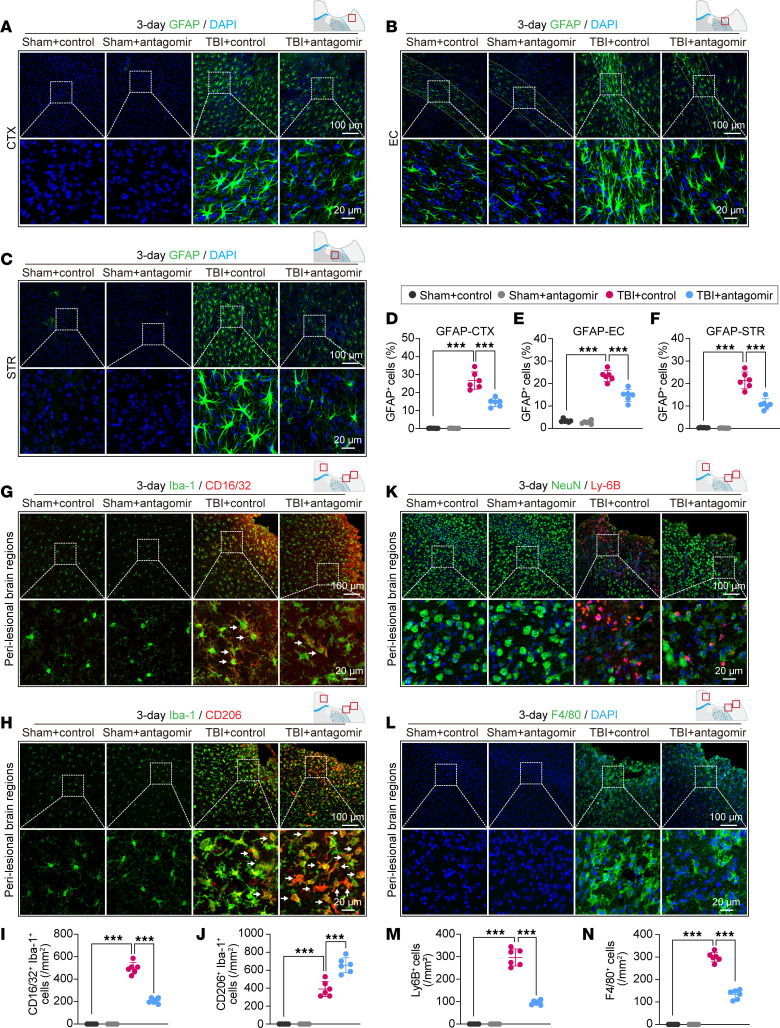
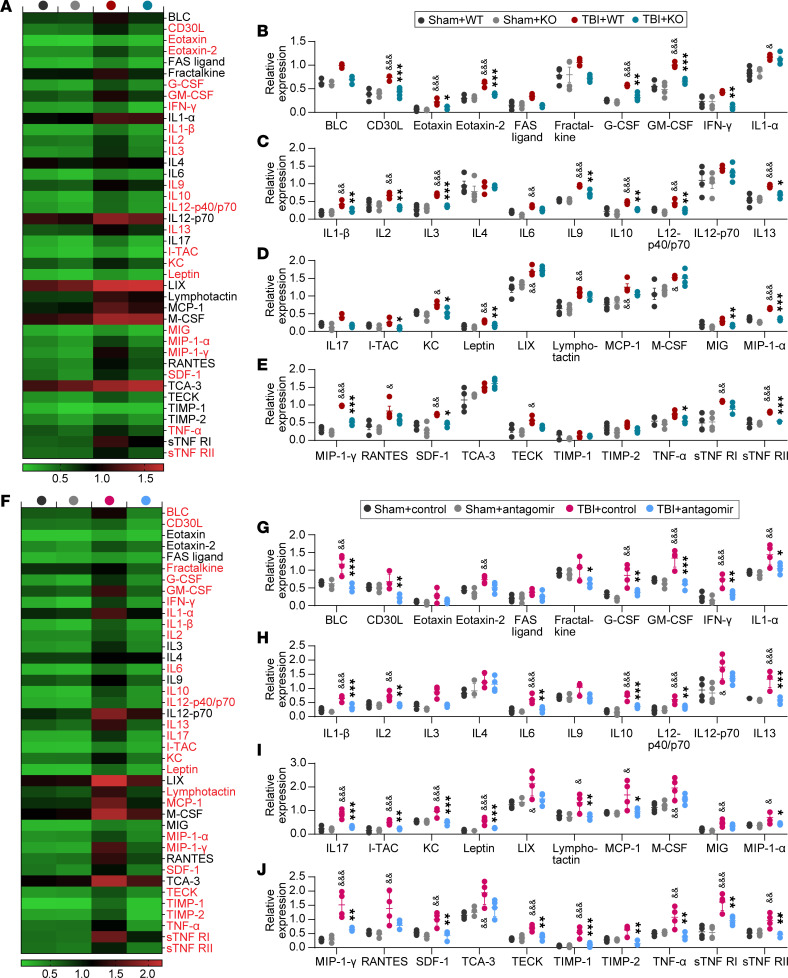
The diffuse axonal damage in white matter and neuronal loss, along with excessive neuroinflammation, hinder long-term functional recovery after traumatic brain injury (TBI). MicroRNAs (miRs) are small noncoding RNAs that negatively regulate protein-coding target genes in a posttranscriptional manner. Recent studies have shown that loss of function of the miR-15a/16-1 cluster reduced neurovascular damage and improved functional recovery in ischemic stroke and vascular dementia. However, the role of the miR-15a/16-1 cluster in neurotrauma is poorly explored. Here, we report that genetic deletion of the miR-15a/16-1 cluster facilitated the recovery of sensorimotor and cognitive functions, alleviated white matter/gray matter lesions, reduced cerebral glial cell activation, and inhibited infiltration of peripheral blood immune cells to brain parenchyma in a murine model of TBI when compared with WT controls. Moreover, intranasal delivery of the miR-15a/16-1 antagomir provided similar brain-protective effects conferred by genetic deletion of the miR-15a/16-1 cluster after experimental TBI, as evidenced by showing improved sensorimotor and cognitive outcomes, better white/gray matter integrity, and less inflammatory responses than the control antagomir-treated mice after brain trauma. miR-15a/16-1 genetic deficiency and miR-15a/16-1 antagomir also significantly suppressed inflammatory mediators in posttrauma brains. These results suggest miR-15a/16-1 as a potential therapeutic target for TBI.
Keywords: Behavior; Demyelinating disorders; Drug therapy; Inflammation; Therapeutics.
Conflict of interest statement
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
