

Treatment of positive catheter tip culture without bloodstream infections in critically ill patients. A case-cohort study from the OUTCOMEREA network
- PMID: 38913096
- PMCID: PMC11245435
- DOI: 10.1007/s00134-024-07498-1
Treatment of positive catheter tip culture without bloodstream infections in critically ill patients. A case-cohort study from the OUTCOMEREA network
Abstract
Purpose: This study aimed to evaluate the impact on subsequent infections and mortality of an adequate antimicrobial therapy within 48 h after catheter removal in intensive care unit (ICU) patients with positive catheter tip culture.
Methods: We performed a retrospective analysis of prospectively collected data from 29 centers of the OUTCOMEREA network. We developed a propensity score (PS) for adequate antimicrobial treatment, based on expert opinion of 45 attending physicians. We conducted a 1:1 case-cohort study matched on the PS score of being adequately treated. A PS-matched subdistribution hazard model was used for detecting subsequent infections and a PS-matched Cox model was used to evaluate the impact of antibiotic therapy on mortality.
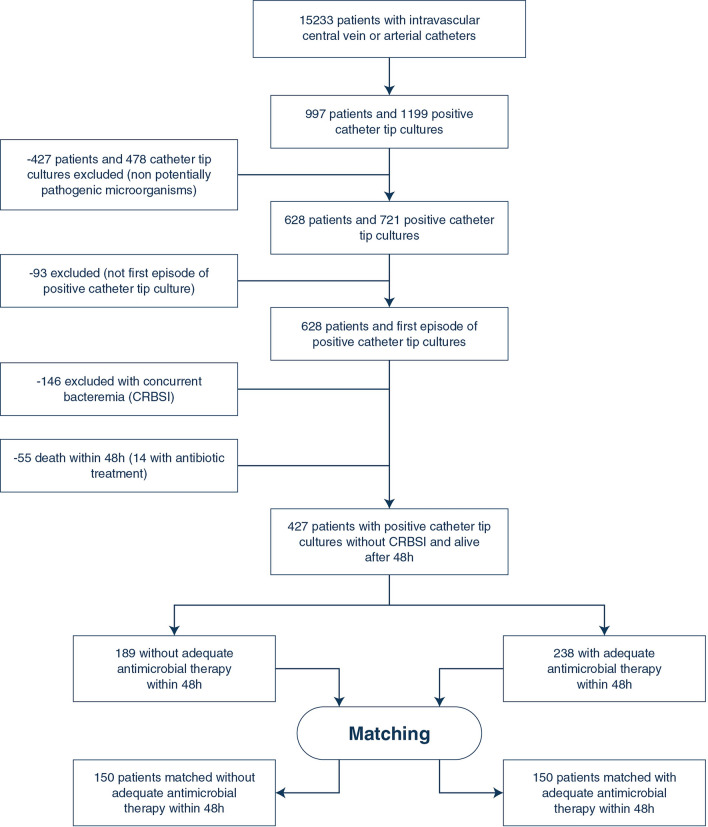
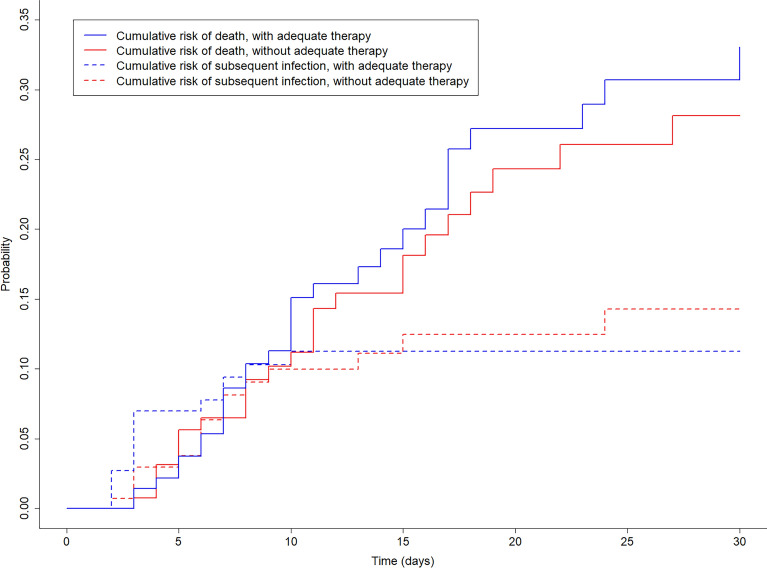
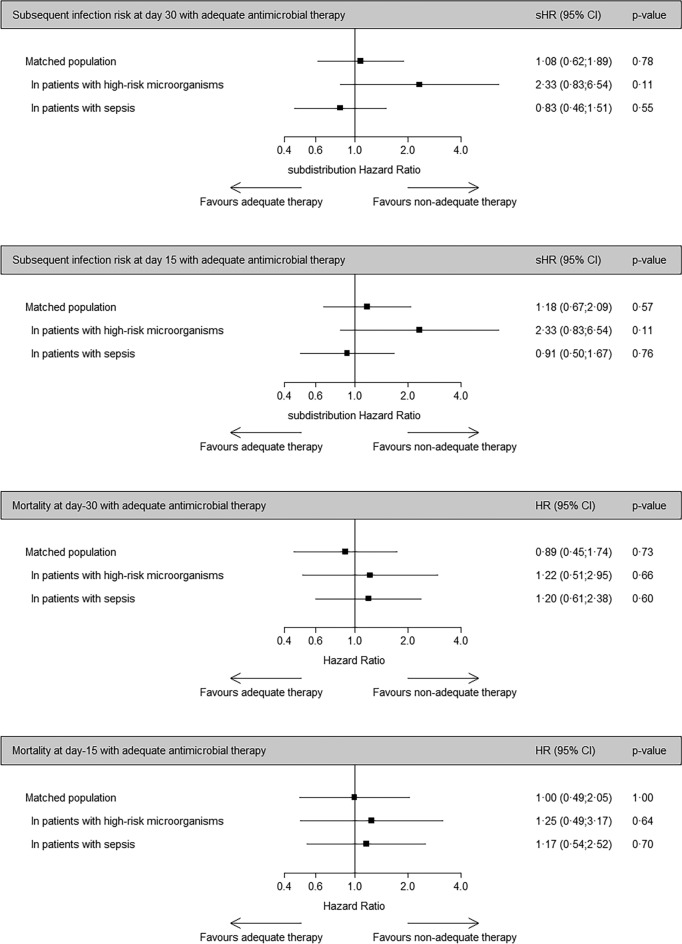
Results: We included 427 patients with a catheter tip culture positive with potentially pathogenic microorganisms. We matched 150 patients with an adequate antimicrobial therapy with 150 controls. In the matched population, 30 (10%) subsequent infections were observed and 62 patients died within 30 days. Using subdistribution hazard models, the daily risk to develop subsequent infection up to Day-30 was similar between treated and non-treated groups (subdistribution hazard ratio [sHR] 1.08, 95% confidence interval [CI] 0.62-1.89, p = 0.78). Using Cox proportional hazard models, the 30-day mortality risk was similar between treated and non-treated groups (HR 0.89, 95% CI 0.45-1.74, p = 0.73).
Conclusions: Antimicrobial therapy was not associated with decreased risk of subsequent infection or death in short-term catheter tip colonization in critically ill patients. Antibiotics may be unnecessary for positive catheter tip cultures.
Keywords: Catheter tip; Catheter-related bloodstream infections; Critically ill; Mortality; Positive catheter tip cultures.
© 2024. The Author(s).
Conflict of interest statement
J-FT reported advisory boards participation for Merck, Gilead, Beckton-Dickinson, Pfizer, Shionogi, Roche diagnostic, Advanz Pharma, research grants from Merck, Pfizer, Thermofischer. MD received support from the “Société de reanimation de langue francaise” and “Groupe de Recherche en Réanimation respiratoire et Onco-hematologique”.
Figures
References
-
- Patel PR, Weiner-Lastinger LM, Dudeck MA, Fike LV, Kuhar DT, Edwards JR, et al. Impact of COVID-19 pandemic on central-line-associated bloodstream infections during the early months of 2020, National Healthcare Safety Network. Infect Control Hosp Epidemiol. 2022;43(6):790–793. doi: 10.1017/ice.2021.108. - DOI - PMC - PubMed
-
- Rosenthal VD, et al. Multinational prospective study of incidence and risk factors for central-line-associated bloodstream infections in 728 intensive care units of 41 Asian, African, Eastern European, Latin American, and Middle Eastern countries over 24 years. Infect Control Hosp Epidemiol. 2023;28:1–11. doi: 10.1017/ice.2023.69. - DOI - PubMed
-
- Adrie C, Garrouste-Orgeas M, Ibn Essaied W, Schwebel C, Darmon M, Mourvillier B, et al. Attributable mortality of ICU-acquired bloodstream infections: impact of the source, causative micro-organism, resistance profile and antimicrobial therapy. J Infect. 2017;74(2):131–141. doi: 10.1016/j.jinf.2016.11.001. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
