

Severe Acute Liver Injury After Hepatotoxic Medication Initiation in Real-World Data
- PMID: 38913369
- PMCID: PMC11197444
- DOI: 10.1001/jamainternmed.2024.1836
Severe Acute Liver Injury After Hepatotoxic Medication Initiation in Real-World Data
Abstract
Importance: Current approaches to classify the hepatotoxic potential of medications are based on cumulative case reports of acute liver injury (ALI), which do not consider the size of the exposed population. There is little evidence from real-world data (data relating to patient health status and/or the delivery of health care routinely collected from sources outside of a research setting) on incidence rates of severe ALI after initiation of medications, accounting for duration of exposure.
Objective: To identify the most potentially hepatotoxic medications based on real-world incidence rates of severe ALI and to examine how these rates compare with categorization based on case reports.
Design, setting, and participants: This series of cohort studies obtained data from the US Department of Veterans Affairs on persons without preexisting liver or biliary disease who initiated a suspected hepatotoxic medication in the outpatient setting between October 1, 2000, and September 30, 2021. Data were analyzed from June 2020 to November 2023.
Exposures: Outpatient initiation of any one of 194 medications with 4 or more published reports of hepatotoxicity.
Main outcomes and measures: Hospitalization for severe ALI, defined by either inpatient: (1) alanine aminotransferase level greater than 120 U/L plus total bilirubin level greater than 2.0 mg/dL or (2) international normalized ratio of 1.5 or higher plus total bilirubin level greater than 2.0 mg/dL recorded within the first 2 days of admission. Acute or chronic liver or biliary disease diagnosis recorded during follow-up or as a discharge diagnosis of a hospitalization for severe ALI resulted in censoring. This study calculated age- and sex-adjusted incidence rates of severe ALI and compared observed rates with hepatotoxicity categories based on cumulative published case reports.
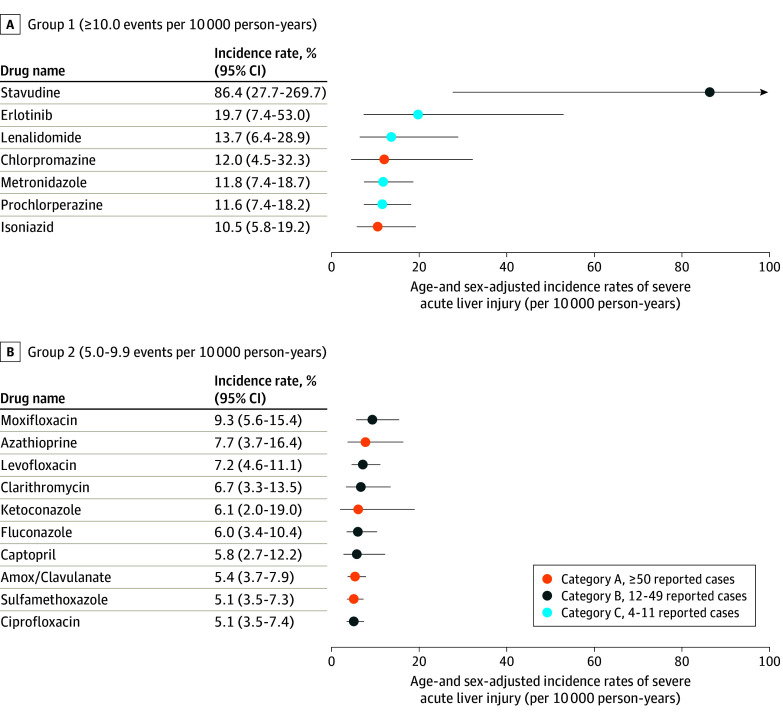
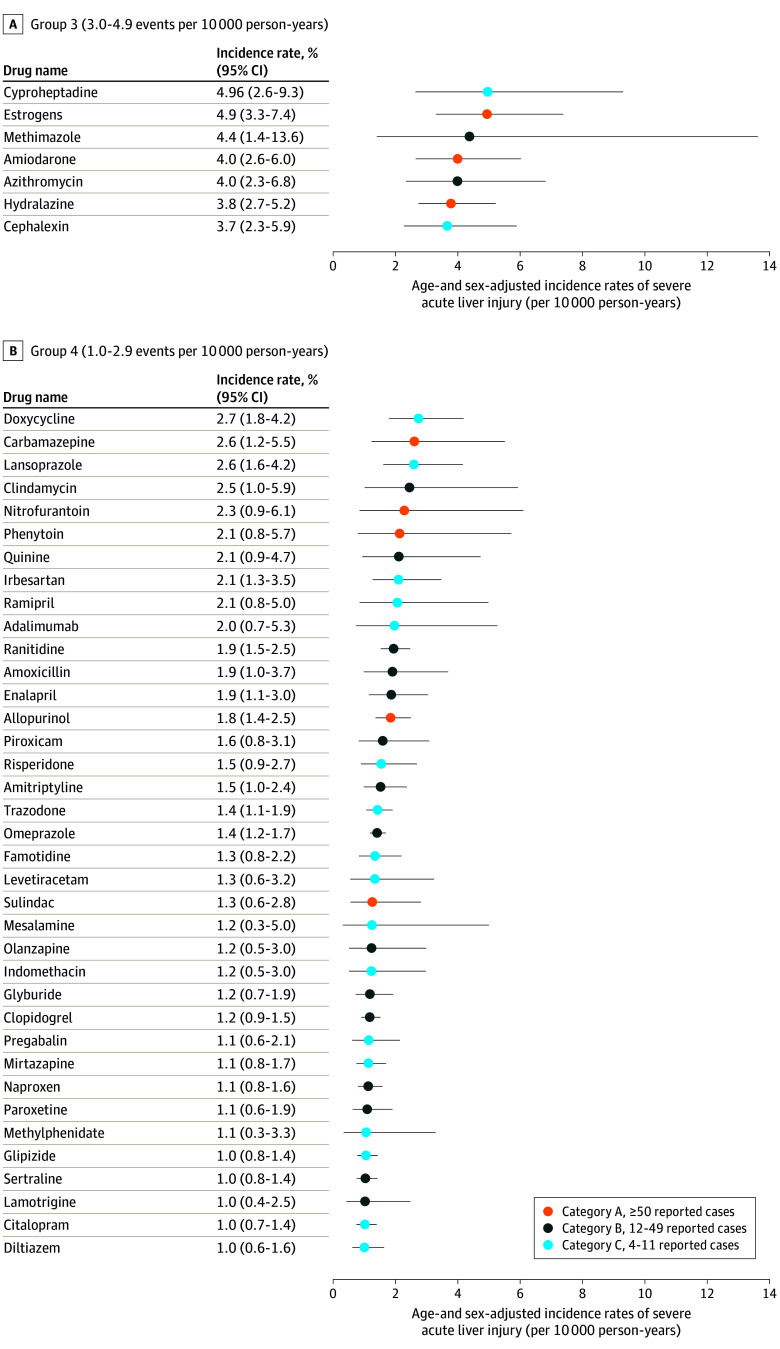
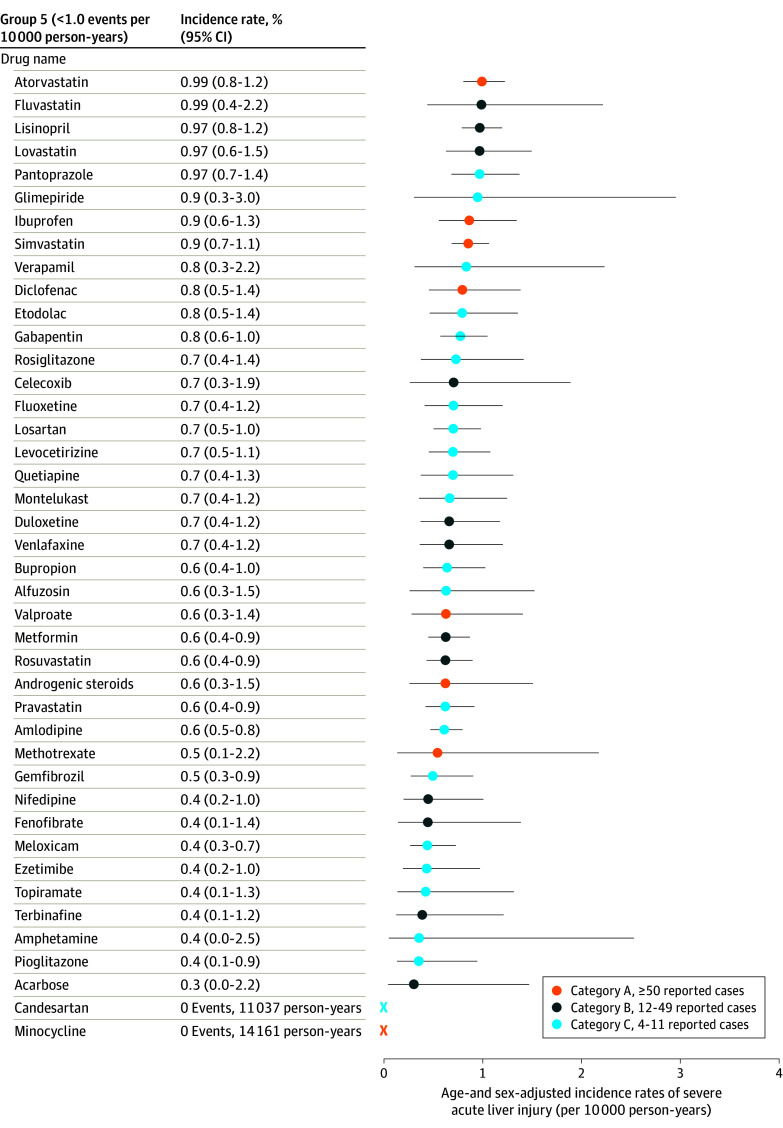
Results: The study included 7 899 888 patients across 194 medication cohorts (mean [SD] age, 64.4 [16.4] years, 7 305 558 males [92.5%], 4 354 136 individuals [55.1%] had polypharmacy). Incidence rates of severe ALI ranged from 0 events per 10 000 person-years (candesartan, minocycline) to 86.4 events per 10 000 person-years (stavudine). Seven medications (stavudine, erlotinib, lenalidomide or thalidomide, chlorpromazine, metronidazole, prochlorperazine, and isoniazid) exhibited rates of 10.0 or more events per 10 000 person-years, and 10 (moxifloxacin, azathioprine, levofloxacin, clarithromycin, ketoconazole, fluconazole, captopril, amoxicillin-clavulanate, sulfamethoxazole-trimethoprim, and ciprofloxacin) had rates between 5.0 and 9.9 events per 10 000 person-years. Of these 17 medications with the highest observed rates of severe ALI, 11 (64%) were not included in the highest hepatotoxicity category when based on case reports.
Conclusions and relevance: In this study, incidence rates of severe ALI using real-world data identified the most potentially hepatotoxic medications and can serve as a tool to investigate hepatotoxicity safety signals obtained from case reports. Case report counts did not accurately reflect the observed rates of severe ALI after medication initiation.
Conflict of interest statement
Figures
Comment on
-
Rethinking Drug-Induced Liver Injury-A New Era of Pharmacovigilance.JAMA Intern Med. 2024 Aug 1;184(8):952-953. doi: 10.1001/jamainternmed.2024.1833. JAMA Intern Med. 2024. PMID: 38913358 No abstract available.
References
-
- National Institute of Diabetes and Digestive and Kidney Diseases . Livertox: clinical and research information on drug-induced liver injury. Updated May 13, 2024. Accessed November 16, 2023. https://www.ncbi.nlm.nih.gov/books/NBK547852/ - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
