

Internet and Telephone Support for Discontinuing Long-Term Antidepressants: The REDUCE Cluster Randomized Trial
- PMID: 38913372
- PMCID: PMC11197448
- DOI: 10.1001/jamanetworkopen.2024.18383
Internet and Telephone Support for Discontinuing Long-Term Antidepressants: The REDUCE Cluster Randomized Trial
Abstract
Importance: There is significant concern regarding increasing long-term antidepressant treatment for depression beyond an evidence-based duration.
Objective: To determine whether adding internet and telephone support to a family practitioner review to consider discontinuing long-term antidepressant treatment is safe and more effective than a practitioner review alone.
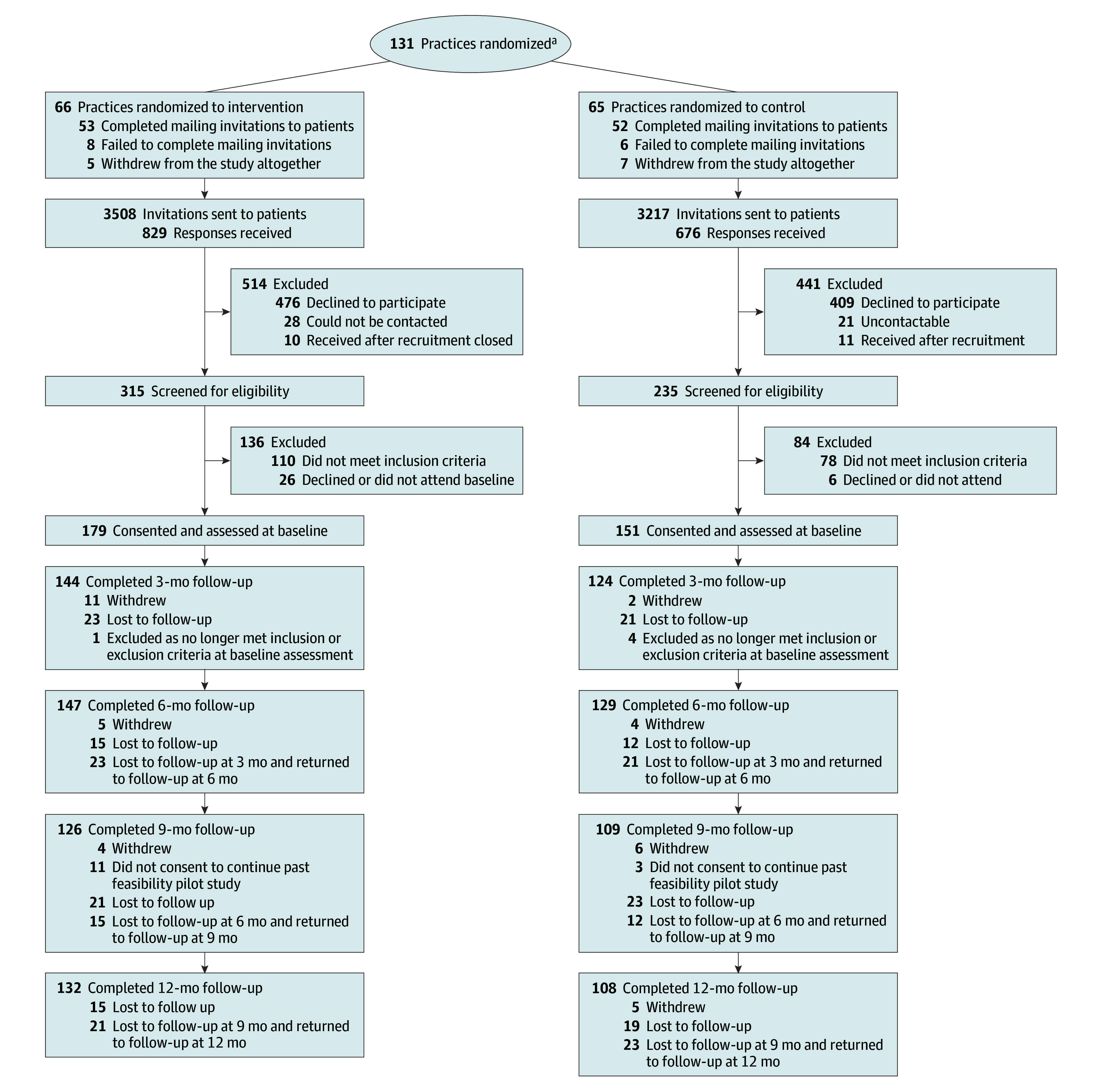
Design, setting, and participants: In this cluster randomized clinical trial, 131 UK family practices were randomized between December 1, 2018, and March 31, 2022, with remote computerized allocation and 12 months of follow-up. Participants and researchers were aware of allocation, but analysis was blind. Participants were adults who were receiving antidepressants for more than 1 year for a first episode of depression or more than 2 years for recurrent depression who were currently well enough to consider discontinuation and wished to do so and who were at low risk of relapse. Of 6725 patients mailed invitations, 330 (4.9%) were eligible and consented.
Interventions: Internet and telephone self-management support, codesigned and coproduced with patients and practitioners.
Main outcomes and measures: The primary (safety) outcome was depression at 6 months (prespecified complete-case analysis), testing for noninferiority of the intervention to under 2 points on the 9-item Patient Health Questionnaire (PHQ-9). Secondary outcomes (testing for superiority) were antidepressant discontinuation, anxiety, quality of life, antidepressant withdrawal symptoms, mental well-being, enablement, satisfaction, use of health care services, and adverse events. Analyses for the main outcomes were performed on a complete-case basis, and multiple imputation sensitivity analysis was performed on an intention-to-treat basis.
Results: Of 330 participants recruited (325 eligible for inclusion; 178 in intervention practices and 147 in control practices; mean [SD] age at baseline, 54.0 [14.9] years; 223 women [68.6%]), 276 (83.6%) were followed up at 6 months, and 240 (72.7%) at 12 months. The intervention proved noninferior; mean (SD) PHQ-9 scores at 6 months were slightly lower in the intervention arm than in the control arm in the complete-case analysis (4.0 [4.3] vs 5.0 [4.7]; adjusted difference, -1.1; 95% CI, -2.1 to -0.1; P = .03) but not significantly different in an intention-to-treat multiple imputation sensitivity analysis (adjusted difference, -0.9 (95% CI, -1.9 to 0.1; P = .08). By 6 months, antidepressants had been discontinued by 66 of 145 intervention arm participants (45.5%) who provided discontinuation data and 54 of 129 control arm participants (41.9%) (adjusted odds ratio, 1.02; 95% CI, 0.52-1.99; P = .96). In the intervention arm, antidepressant withdrawal symptoms were less severe, and mental well-being was better compared with the control arm; differences were small but significant. There were no significant differences in the other outcomes; 28 of 179 intervention arm participants (15.6%) and 22 of 151 control arm participants (14.6%) experienced adverse events.
Conclusions and relevance: In this cluster randomized clinical trial of adding internet and telephone support to a practitioner review for possible antidepressant discontinuation, depression was slightly better with support, but the rate of discontinuation of antidepressants did not significantly increase. Improvements in antidepressant withdrawal symptoms and mental well-being were also small. There were no significant harms. Family practitioner review for possible discontinuation of antidepressants appeared safe and effective for more than 40% of patients willing and well enough to discontinue.
Trial registration: ISRCTN registry Identifiers: ISRCTN15036829 (internal pilot trial) and ISRCTN12417565 (main trial).
Conflict of interest statement
Figures
References
-
- Taylor S, Annand F, Burkinshaw P, et al. . Dependence and Withdrawal Associated With Some Prescribed Medicines: An Evidence Review. Public Health England; 2019.
