

Surgical Outcomes and Genomic Insights of Nonclear Cell Renal Cell Carcinoma With Synchronous and Metachronous Nodal Disease
- PMID: 38913557
- PMCID: PMC11335441
- DOI: 10.1097/UPJ.0000000000000623
Surgical Outcomes and Genomic Insights of Nonclear Cell Renal Cell Carcinoma With Synchronous and Metachronous Nodal Disease
Abstract
Introduction: Oncological outcomes in patients with nonclear cell renal cell carcinoma (non-ccRCC) treated with surgery for locoregional nodal disease (ND) remain incompletely characterized. The objective was to investigate the characteristics and outcomes of non-ccRCC patients treated with lymph node dissection (LND) and salvage-LND (S-LND).
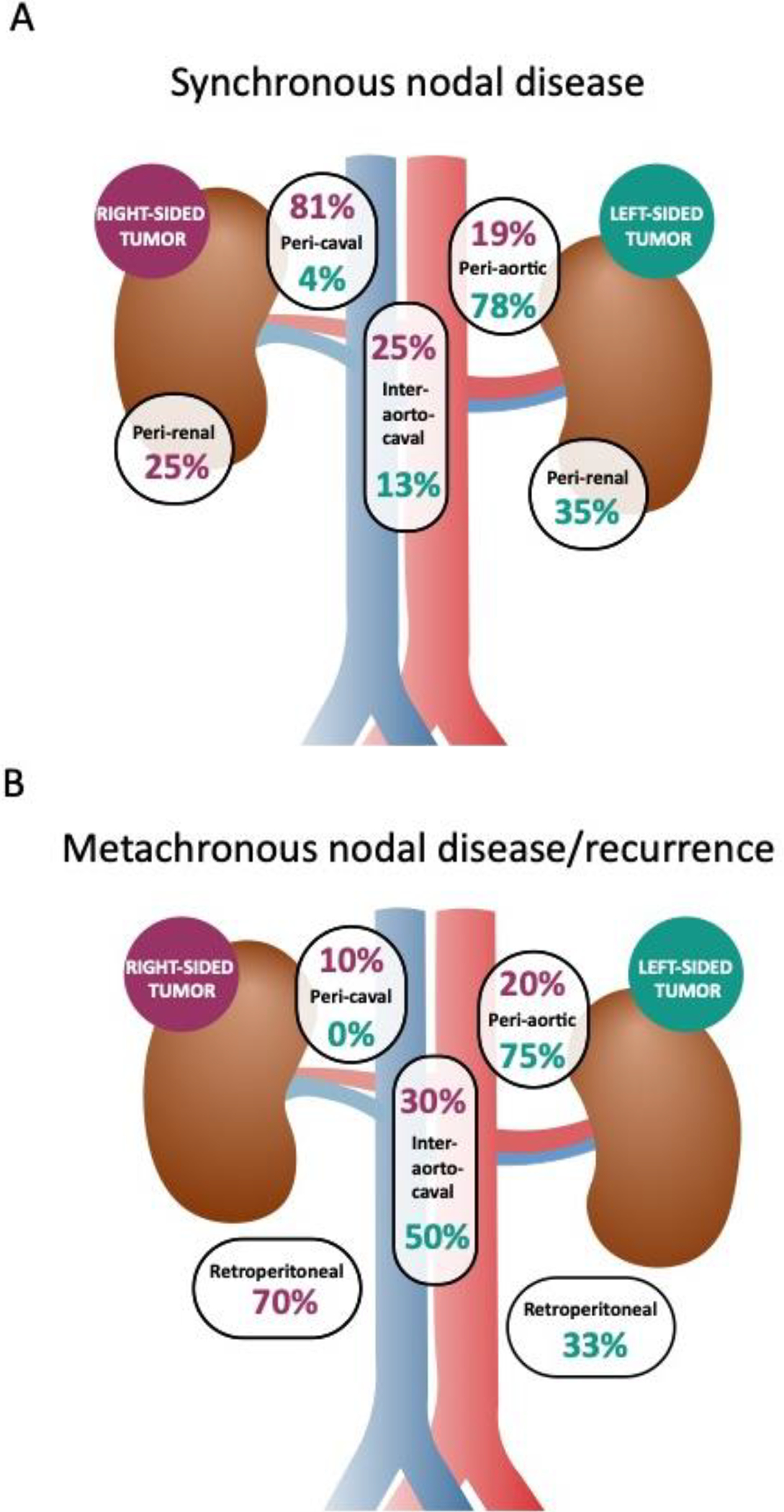
Methods: A total of 1627 patients underwent nephrectomy for nonmetastatic non-ccRCC at Memorial Sloan Kettering Cancer Center between 2007 and 2023. Histology was grouped as papillary, chromophobe, unclassified, and rare subtypes. Retrospective evaluation identified 2.5% (n = 40) of patients with nodal disease at time of nephrectomy (synchronous-ND) and 1.1% (n = 18) with metachronous nodal disease limited to the retroperitoneum (metachronous-ND). Patients' demographics and tumor characteristics were recorded and evaluated by univariate and multivariate cox regression models. Recurrence-free survival (RFS) and overall survival (OS) were estimated by the Kaplan-Meier method. Patients who underwent tumor DNA sequencing during their clinical course were considered for genomic analysis.
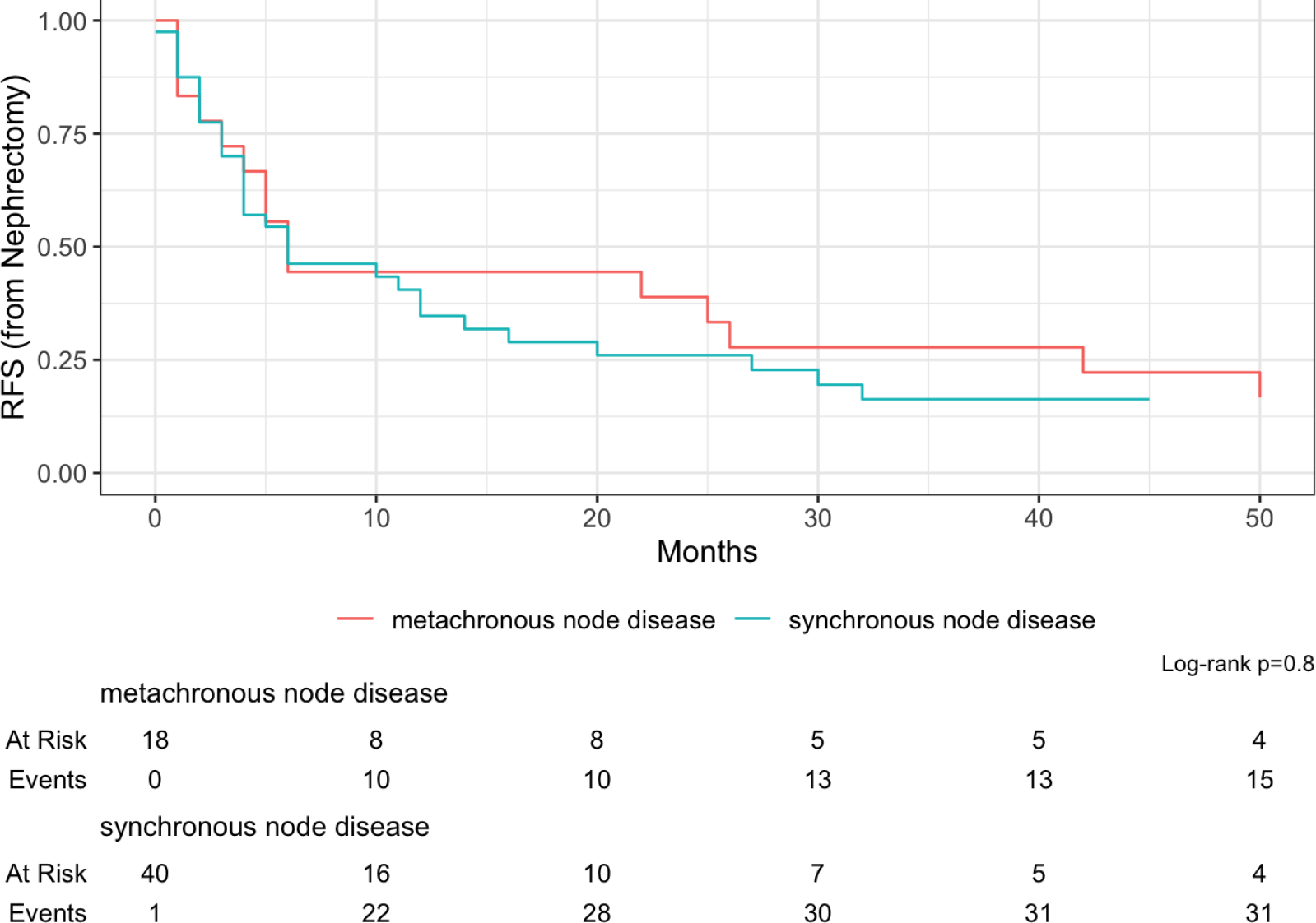
Results: OS trended toward longer in metachronous-ND (51 vs 105 months; P = .2), though 23% of patients with synchronous-ND were recurrence-free at 45 months median follow-up. In multivariate analysis, rare histologies were associated with decreased OS (P = .030) and metachronous-ND with improved OS (P = .036). RFS and OS after S-LND was 15 and 96 months, respectively. Late onset of metachronous-ND/recurrence was associated with improved OS (P = .008). Genetic alterations in SETD2, TP53, B2M, and FGFR3 were exclusively seen in synchronous-ND, and tumor mutation burden (TMB) was also higher in patients with synchronous-ND (P = .016).
Conclusions: Patients with metachronous-ND tend to have prolonged OS compared to synchronous-ND, but a substantial portion of patients with synchronous-ND still enter a durable disease-free state following LND. S-LND can likewise provide long-term survival, particularly in patients with longer time to metachronous nodal recurrence. Synchronous-ND was associated with SETD2, TP53, and NF2 alteration as well as higher TMB.
Keywords: lymph node excision; nephrectomy; renal cell carcinoma.
Figures




Comment in
-
Editorial Commentary.Urol Pract. 2024 Sep;11(5):869-870. doi: 10.1097/UPJ.0000000000000627. Epub 2024 Jun 5. Urol Pract. 2024. PMID: 38913562 No abstract available.
References
-
- Chen Y-B, Xu J, Skanderup AJ, Dong Y, Brannon AR, Wang L, Won HH, Wang PI, Nanjangud GJ, Jungbluth AA, Li W, Ojeda V, Hakimi AA, Voss MH, Schultz N, Motzer RJ, Russo P, Cheng EH, Giancotti FG, Lee W, Berger MF, Tickoo SK, Reuter VE, and Hsieh JJ, Molecular analysis of aggressive renal cell carcinoma with unclassified histology reveals distinct subsets. Nature Communications, 2016. 7(1): p. 13131. 10.1038/ncomms13131 - DOI - PMC - PubMed
-
- Lee CA-O, Voss MA-O, Carlo MA-O, Chen YA-O, Zucker MA-OX, Knezevic AA-O, Lefkowitz RA, Shapnik N, Dadoun C, Reznik EA-O, Shah NA-O, Owens CN, McHugh DA-O, Aggen DA-O, Laccetti AL, Kotecha RA-O, Feldman DA-O, and Motzer RA-O, Phase II Trial of Cabozantinib Plus Nivolumab in Patients With Non-Clear-Cell Renal Cell Carcinoma and Genomic Correlates. (1527–7755 (Electronic)), - PMC - PubMed
-
- Ljungberg B, Albiges L, Abu-Ghanem Y, Bedke J, Capitanio U, Dabestani S, Fernández-Pello S, Giles RH, Hofmann F, Hora M, Klatte T, Kuusk T, Lam TB, Marconi L, Powles T, Tahbaz R, Volpe A, and Bex A, European Association of Urology Guidelines on Renal Cell Carcinoma: The 2022 Update. (1873–7560 (Electronic)), - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
