

Efficacy and Safety of Remdesivir in People With Impaired Kidney Function Hospitalized for COVID-19 Pneumonia: A Randomized Clinical Trial
- PMID: 38913574
- PMCID: PMC11581693
- DOI: 10.1093/cid/ciae333
Efficacy and Safety of Remdesivir in People With Impaired Kidney Function Hospitalized for COVID-19 Pneumonia: A Randomized Clinical Trial
Abstract
Background: Few antiviral therapies have been studied in patients with coronavirus disease 2019 (COVID-19) and kidney impairment. Herein, the efficacy, safety, and pharmacokinetics of remdesivir, its metabolites, and sulfobutylether-β-cyclodextrin excipient were evaluated in hospitalized patients with COVID-19 and severe kidney impairment.
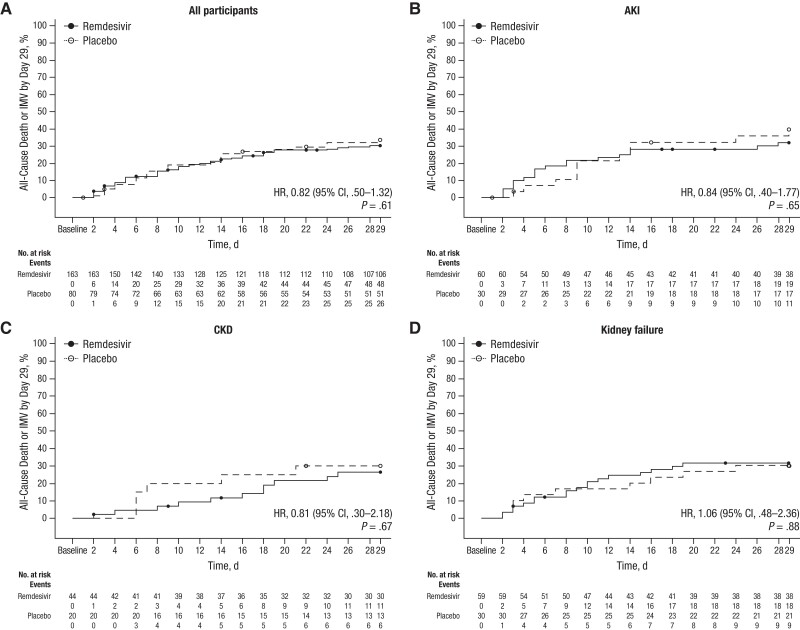
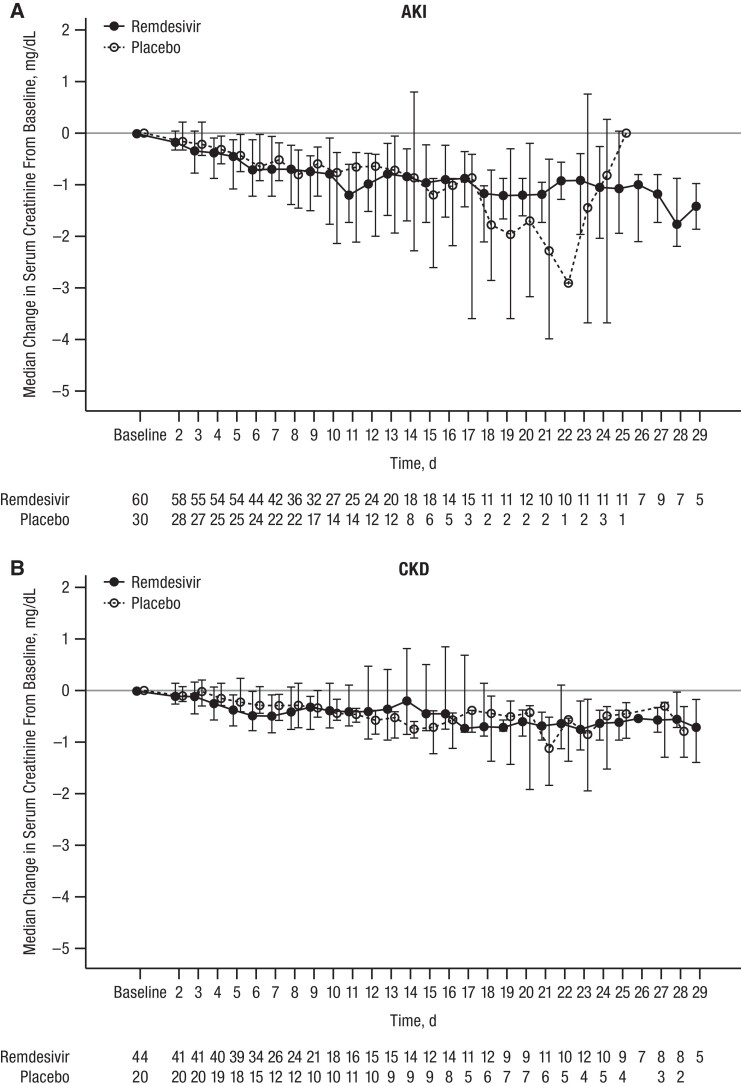
Methods: In REDPINE, a phase 3, randomized, double-blind, placebo-controlled study, participants aged ≥12 years hospitalized for COVID-19 pneumonia with acute kidney injury, chronic kidney disease, or kidney failure were randomized 2:1 to receive intravenous remdesivir (200 mg on day 1; 100 mg daily up to day 5) or placebo (enrollment from March 2021 to March 2022). The primary efficacy end point was the composite of the all-cause mortality rate or invasive mechanical ventilation rate through day 29. Safety was evaluated through day 60.
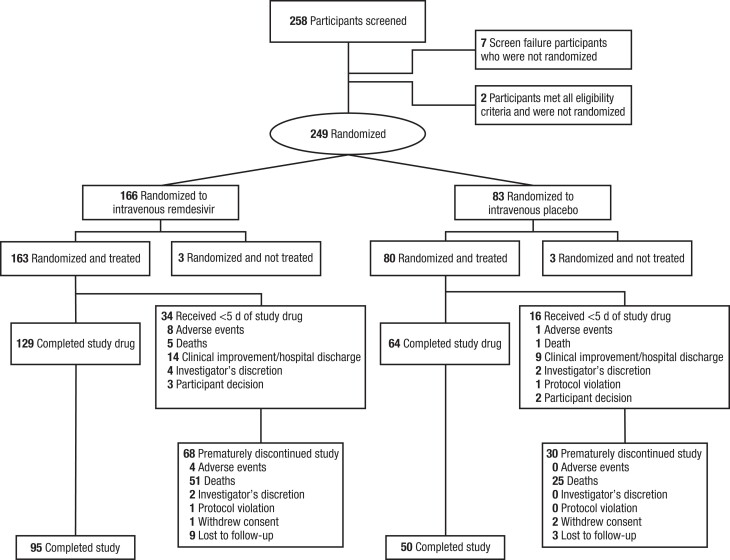
Results: Although enrollment concluded early, 243 participants were enrolled and treated (remdesivir, n = 163; placebo, n = 80). At baseline, 90 participants (37.0%) had acute kidney injury (remdesivir, n = 60; placebo, n = 30), 64 (26.3%) had chronic kidney disease (remdesivir, n = 44; placebo, n = 20), and 89 (36.6%) had kidney failure (remdesivir, n = 59; placebo, n = 30); and 31 (12.8%) were vaccinated against COVID-19. Composite all-cause mortality or invasive mechanical ventilation rates through day 29 were 29.4% and 32.5% in the remdesivir and placebo group, respectively (P = .61). Treatment-emergent adverse events were reported in 80.4% for remdesivir versus 77.5% for placebo, and serious adverse events in 50.3% versus 50.0%, respectively. Pharmacokinetic plasma exposure to remdesivir was not affected by kidney function.
Conclusions: Although the study was underpowered, no significant difference in efficacy was observed between treatment groups. REDPINE demonstrated that remdesivir is safe in patients with COVID-19 and severe kidney impairment.
Clinical trials registration: EudraCT 2020-005416-22; Clinical Trials.gov NCT04745351.
Keywords: COVID-19; SARS-CoV-2; kidney impairment; remdesivir.
© The Author(s) 2024. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest . M. E. S. received research funding from Gilead Sciences, EMD Serono, AbbVie, Angion, Novartis, Merck, Cabaletta Bio, and Otsuka; served as a scientific advisory board member for Travere, Novartis, Vera Therapeutics, Calliditas, and Mallinckrodt; and served as a data and safety monitoring board member for Alpine Immunoscience. J. R. S. received research funding, consulting fees, and lecture sponsorships from and served on advisory boards for Gilead Sciences, GSK, Janssen-Cilag, Bristol Myers Squibb, ViiV Healthcare, and Merck Sharp & Dohme (MSD). J. D. G. consulted for Gilead Sciences, Eli Lilly, GSK, and Karius; received research support or grants from Gilead Sciences, Eli Lilly, Regeneron, and MSD (Biomedical Advanced Research and Development Authority); and received nonfinancial support from Adaptive Biotechnologies, Monogram Biosciences, and Labcorp (outside the current study). J. P. T. is a consultant for Outset Medical and owns stock and/or stock options in Novo Nordisk A/S. Y. K., J. L., S. R., Y. Z., H. H., R. H. H., A. O., and H. W. are stockholders and employees of Gilead Sciences. R. H. is a former employee and stockholder of Gilead Sciences. H. N. H. received consulting fees from Gilead Sciences. R. L. G. served as a consultant for AbbVie, AstraZeneca, Eli Lilly, GSK, Gilead Sciences, Johnson & Johnson, Roivant Sciences, and Roche Pharmaceuticals; served as a national coordinating primary investigator for Johnson & Johnson; served on an academic steering committee for Roivant Sciences; received from Gilead Sciences a gift in kind to Baylor Scott & White Research Institute to facilitate NCT03383419; owns de minimis stock in AbCellera Biologics; and served as a speaker for Pfizer, outside the scope of coronavirus disease 2019 (COVID-19). D. N. F. served on a Gilead Sciences advisory board, outside the scope of COVID-19, and served as a site primary investigator for clinical trials with Gilead Sciences, Regeneron, and MetroBiotech. R. B. served on a scientific advisory board for AstraZeneca, Bayer, Boehringer Ingelheim, MSD, and Mundipharma; and served as a speaker for AstraZeneca, Bayer, MSD, Mundipharma, and Gilead Sciences, outside the scope of COVID-19. C. B. S. has received research support from Gilead Sciences, MSD, GSK, Takeda, Shire, Janssen, AbbVie, and ViiV Healthcare. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- VEKLURY® (remdesivir) [prescribing information] . Foster City, CA: Gilead Sciences, 2022.
