

Trends in weight gain recorded in English primary care before and during the Coronavirus-19 pandemic: An observational cohort study using the OpenSAFELY platform
- PMID: 38913709
- PMCID: PMC11249215
- DOI: 10.1371/journal.pmed.1004398
Trends in weight gain recorded in English primary care before and during the Coronavirus-19 pandemic: An observational cohort study using the OpenSAFELY platform
Abstract
Background: Obesity and rapid weight gain are established risk factors for noncommunicable diseases and have emerged as independent risk factors for severe disease following Coronavirus Disease 2019 (COVID-19) infection. Restrictions imposed to reduce COVID-19 transmission resulted in profound societal changes that impacted many health behaviours, including physical activity and nutrition, associated with rate of weight gain. We investigated which clinical and sociodemographic characteristics were associated with rapid weight gain and the greatest acceleration in rate of weight gain during the pandemic among adults registered with an English National Health Service (NHS) general practitioner (GP) during the COVID-19 pandemic.
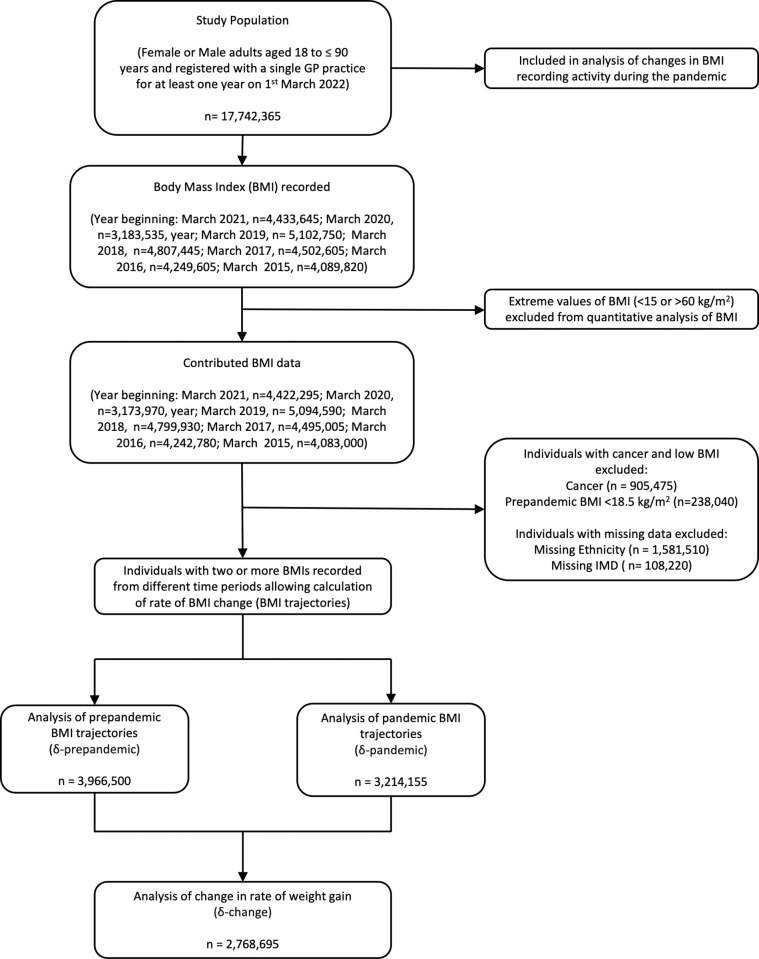
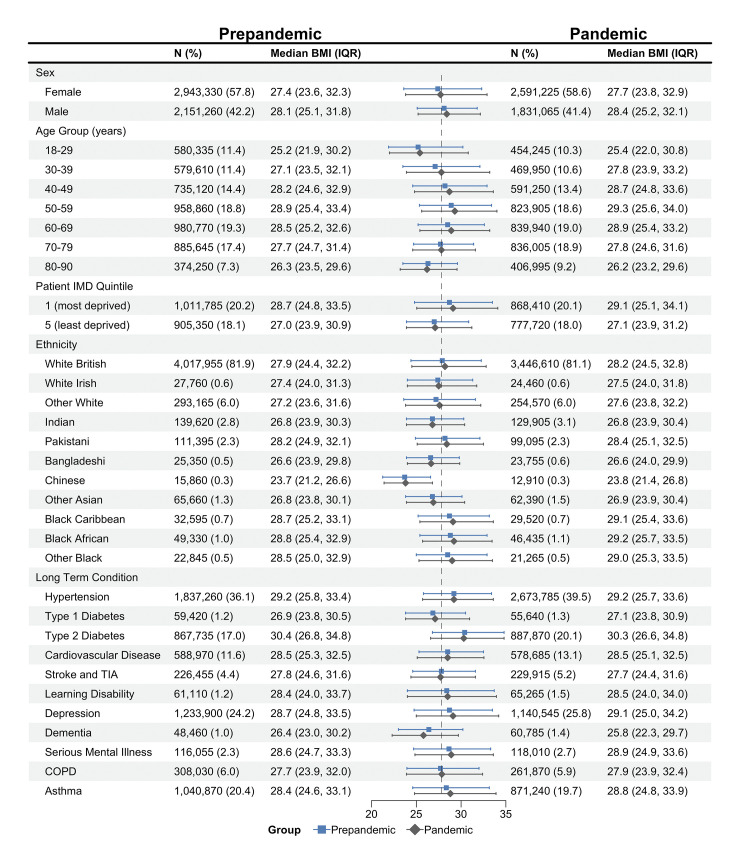
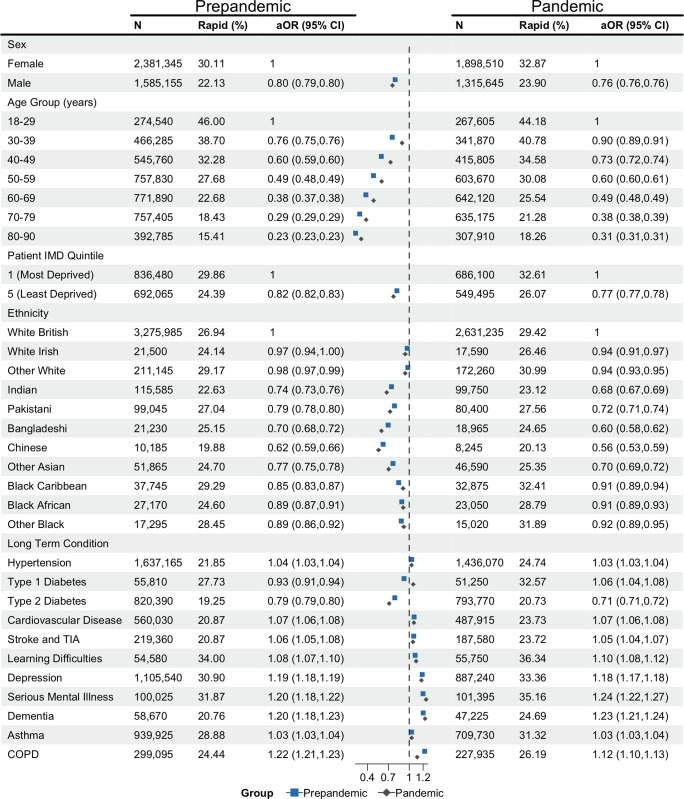
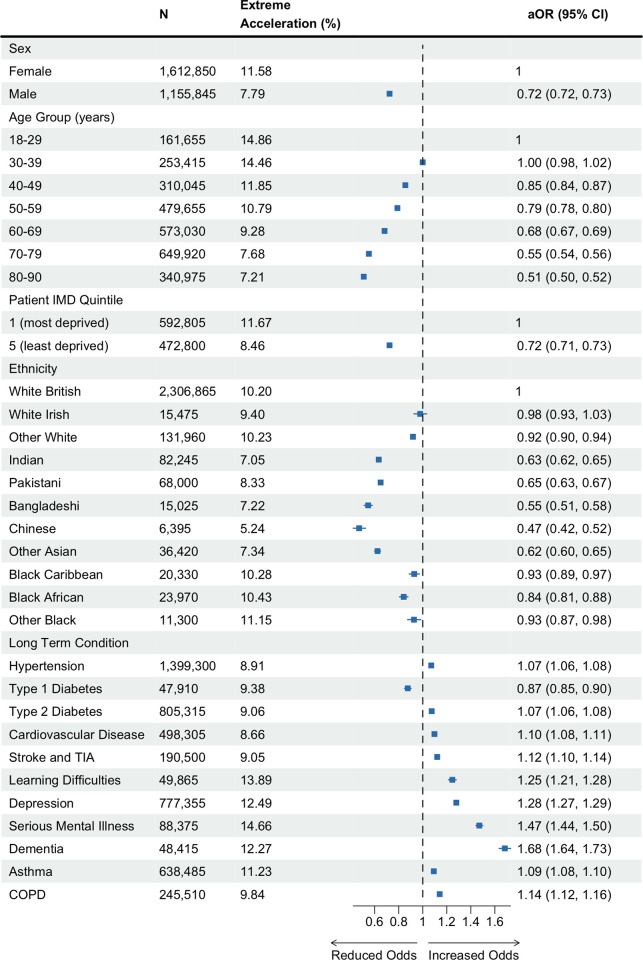
Methods and findings: With the approval of NHS England, we used the OpenSAFELY platform inside TPP to conduct an observational cohort study of routinely collected electronic healthcare records. We investigated changes in body mass index (BMI) values recorded in English primary care between March 2015 and March 2022. We extracted data on 17,742,365 adults aged 18 to 90 years old (50.1% female, 76.1% white British) registered with an English primary care practice. We estimated individual rates of weight gain before (δ-prepandemic) and during (δ-pandemic) the pandemic and identified individuals with rapid weight gain (>0.5 kg/m2/year) in each period. We also estimated the change in rate of weight gain between the prepandemic and pandemic period (δ-change = δ-pandemic-δ-prepandemic) and defined extreme accelerators as the 10% of individuals with the greatest increase in their rate of weight gain (δ-change ≥1.84 kg/m2/year) between these periods. We estimated associations with these outcomes using multivariable logistic regression adjusted for age, sex, index of multiple deprivation (IMD), and ethnicity. P-values were generated in regression models. The median BMI of our study population was 27.8 kg/m2, interquartile range (IQR) [24.3, 32.1] in 2019 (March 2019 to February 2020) and 28.0 kg/m2, IQR [24.4, 32.6] in 2021. Rapid pandemic weight gain was associated with sex, age, and IMD. Male sex (male versus female: adjusted odds ratio (aOR) 0.76, 95% confidence interval (95% CI) [0.76, 0.76], p < 0.001), older age (e.g., 50 to 59 years versus 18 to 29 years: aOR 0.60, 95% CI [0.60, 0.61], p < 0.001]); and living in less deprived areas (least-deprived-IMD-quintile versus most-deprived: aOR 0.77, 95% CI [0.77, 0.78] p < 0.001) reduced the odds of rapid weight gain. Compared to white British individuals, all other ethnicities had lower odds of rapid pandemic weight gain (e.g., Indian versus white British: aOR 0.69, 95% CI [0.68, 0.70], p < 0.001). Long-term conditions (LTCs) increased the odds, with mental health conditions having the greatest effect (e.g., depression (aOR 1.18, 95% CI [1.17, 1.18], p < 0.001)). Similar characteristics increased odds of extreme acceleration in the rate of weight gain between the prepandemic and pandemic periods. However, changes in healthcare activity during the pandemic may have introduced new bias to the data.
Conclusions: We found female sex, younger age, deprivation, white British ethnicity, and mental health conditions were associated with rapid pandemic weight gain and extreme acceleration in rate of weight gain between the prepandemic and pandemic periods. Our findings highlight the need to incorporate sociodemographic, physical, and mental health characteristics when formulating research, policies, and interventions targeting BMI in the period of post pandemic service restoration and in future pandemic planning.
Copyright: © 2024 Samuel et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
MS salary costs have been supported through a National Institute for Health and Care Research (NIHR) funded academic clinical fellowship in primary care (ACF-2017-19-006) and NIHR grant funding (NIHR AI-MULTIPLY Consortium NIHR203982) https://www.nihr.ac.uk/. RYP is supported by the EPSRC Centre for Doctoral Training in Health Data Science (EP/S02428X/1). RYP was previously employed as a data scientist for the Bennet Institute which is funded by grants from the Bennett Foundation, Wellcome Trust, NIHR Oxford Biomedical Research Centre, NIHR Applied Research Collaboration Oxford and Thames Valley, Mohn-Westlake Foundation. SVE has been funded by a Diabetes UK Sir George Alberti research training fellowship (grant number: 17/0005588) and University College London Hospitals Biomedical Research Centre, Cardiovascular theme. FE salary cost is supported by MRC (MR/S027297/1) “Multimorbidity, clusters, trajectories and genetic risk in British south Asians, 2020-2023”. DS is funded by the NIHR (NIHR203982). AM is a senior clinical researcher at the University of Oxford in the Bennett Institute, which is funded by grants from the Bennett Foundation, Wellcome Trust, NIHR Oxford Biomedical Research Centre, NIHR Applied Research Collaboration Oxford and Thames Valley, Mohn-Westlake Foundation. AM has consulted for https://inductionhealthcare.com/. AM has represented the RCGP in the health informatics group and the Professional Advisory Group that advises on access to GP Data for Pandemic Planning and Research (GDPPR); the latter role is paid. AM is a former employee and Chief Medical Officer of NHS Digital (having left NHS Digital in January 2020). AM has consulted for health care vendors, the last time in 2022; the companies consulted in the last 3 years have no relationship to OpenSAFELY. RM is supported by Barts Charity (MGU0504). JV was the National Clinical Director for Diabetes and Obesity at National Health Service (NHS) England from April 2013 to September 2023 and is funded by the Imperial National Institute for Health Research (NIHR) Biomedical Research Centre and North-West London NIHR Applied Research Collaboration. BMK is also employed by NHS England. KK is supported by the National Institute for Health Research (NIHR) Applied Research Collaboration East Midlands (ARC EM) and the NIHR Leicester Biomedical Research Centre (BRC). KK has acted as a consultant, speaker or received grants for investigator-initiated studies for Astra Zeneca, Bayer, Novartis, Novo Nordisk, Sanofi-Aventis, Lilly and Merck Sharp & Dohme, Boehringer Ingelheim, Oramed Pharmaceuticals, Roche and Applied Therapeutics. SF has received grants from the NIHR (NIHR 31672, NIHR 202635) and MRC (MR/W014416/1, MR/V004905/1, MR/S027297/1). SF, RM, CM are part of the Genes & Health programme, which is part-funded (including salary contributions) by a Life Sciences Consortium comprising Astra Zeneca PLC, Bristol-Myers Squibb Company, GlaxoSmithKline Research and Development Limited, Maze Therapeutics Inc, Merck Sharp & Dohme LLC, Novo Nordisk A/S, Pfizer Inc, Takeda Development Centre Americas Inc. This research used data assets made available as part of the Data and Connectivity National Core Study, led by Health Data Research UK in partnership with the Office for National Statistics and funded by UK Research and Innovation (grant ref MC_PC_20058). In addition, the OpenSAFELY Platform is supported by grants from the Wellcome Trust (222097/Z/20/Z); MRC (MR/V015757/1, MC_PC-20059, MR/W016729/1); NIHR (NIHR135559, COV-LT2-0073), and Health Data Research UK (HDRUK2021.000, 2021.0157).
Figures
References
-
- Cheng YJ, Chen ZG, Wu SH, Mei WY, Yao FJ, Zhang M, et al.. Body mass index trajectories during mid to late life and risks of mortality and cardiovascular outcomes: Results from four prospective cohorts. EClinicalMedicine. 2021;33:100790. Epub 20210318. doi: 10.1016/j.eclinm.2021.100790 ; PubMed Central PMCID: PMC7985466. - DOI - PMC - PubMed
-
- Mathur R, Rentsch CT, Morton CE, Hulme WJ, Schultze A, MacKenna B, et al.. Ethnic differences in SARS-CoV-2 infection and COVID-19-related hospitalisation, intensive care unit admission, and death in 17 million adults in England: an observational cohort study using the OpenSAFELY platform. Lancet. 2021;397(10286):1711–24. Epub 20210430. doi: 10.1016/S0140-6736(21)00634-6 ; PubMed Central PMCID: PMC8087292. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
