

Projecting the Potential Clinical and Economic Impact of HIV Prevention Resource Reallocation in Tennessee
- PMID: 38913762
- PMCID: PMC11650892
- DOI: 10.1093/cid/ciae243
Projecting the Potential Clinical and Economic Impact of HIV Prevention Resource Reallocation in Tennessee
Abstract
Background: In 2023, Tennessee replaced $6.2 M in US Centers for Disease Control and Prevention (CDC) human immunodeficiency virus (HIV) prevention funding with state funds to redirect support away from men who have sex with men (MSM), transgender women (TGW), and heterosexual Black women (HSBW) and to prioritize instead first responders (FR), pregnant people (PP), and survivors of sex trafficking (SST).
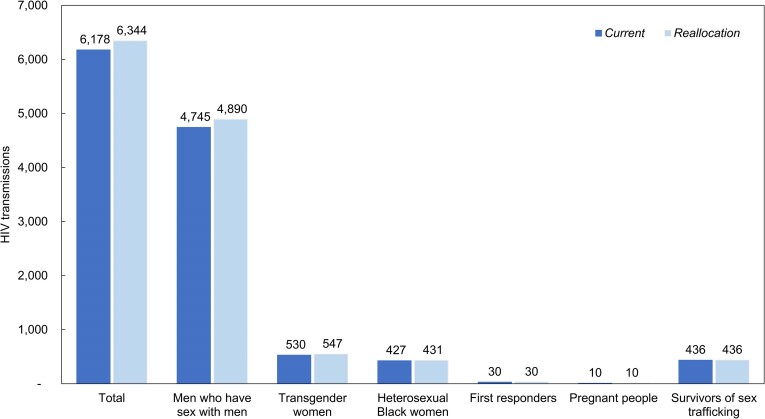
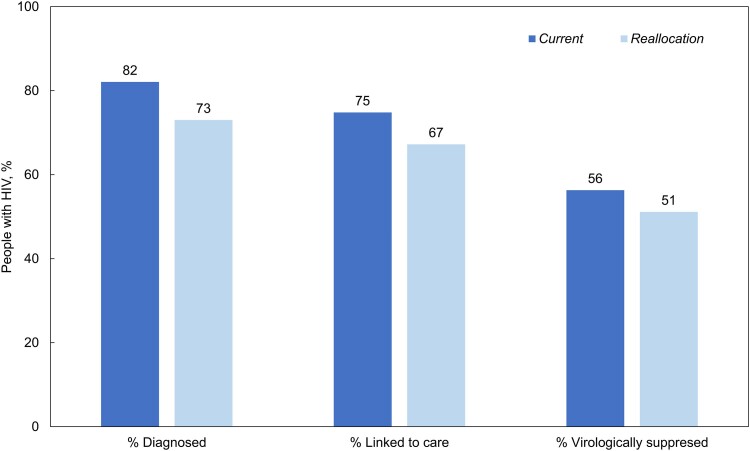
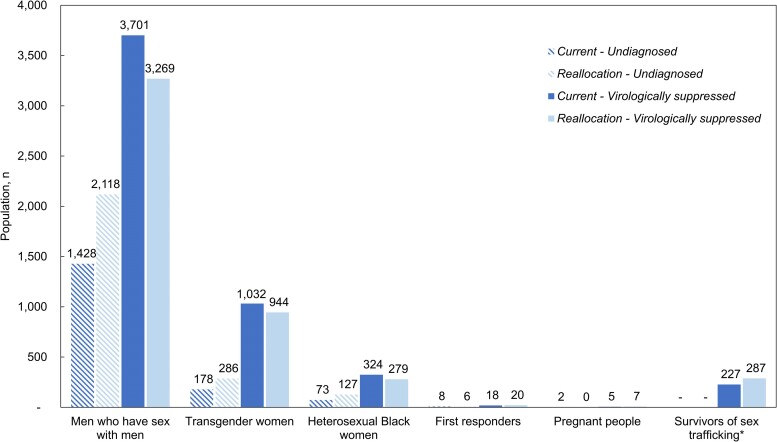
Methods: We used a simulation model of HIV disease to compare the clinical impact of Current, the present allocation of condoms, preexposure prophylaxis (PrEP), and HIV testing to CDC priority risk groups (MSM/TGW/HSBW); with Reallocation, funding instead increased HIV testing and linkage of Tennessee-determined priority populations (FR/PP/SST). Key model inputs included baseline condom use (45%-49%), PrEP provision (0.1%-8%), HIV testing frequency (every 2.5-4.8 years), and 30-day HIV care linkage (57%-65%). We assumed Reallocation would reduce condom use (-4%), PrEP provision (-26%), and HIV testing (-47%) in MSM/TGW/HSBW, whereas it would increase HIV testing among FR (+47%) and HIV care linkage (to 100%/90%) among PP/SST.
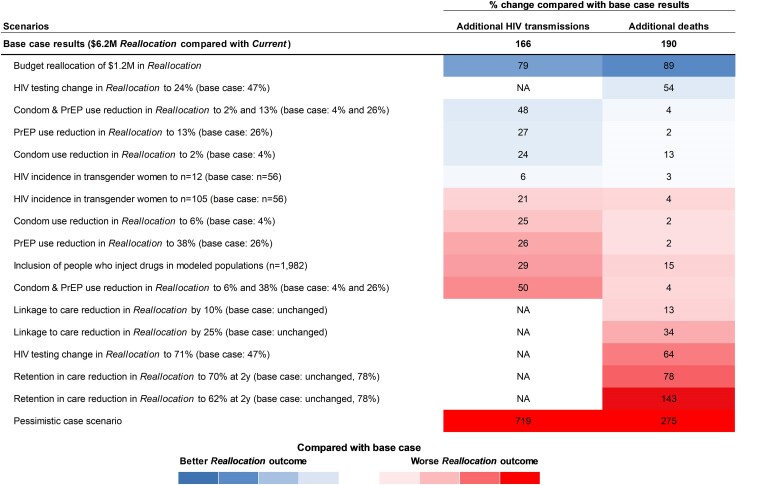
Results: Reallocation would lead to 166 additional HIV transmissions, 190 additional deaths, and 843 life-years lost over 10 years. HIV testing reductions were most influential in sensitivity analysis; even a 24% reduction would result in 287 more deaths compared to Current. With pessimistic assumptions, we projected 1359 additional HIV transmissions, 712 additional deaths, and 2778 life-years lost over 10 years.
Conclusions: Redirecting HIV prevention funding in Tennessee would greatly harm CDC priority populations while conferring minimal benefits to new priority populations.
Keywords: HIV; HIV prevention; HIV prevention resource allocation; Health policy; Tennessee HIV prevention.
© The Author(s) 2024. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest . A. L. A. discloses participation on the advisory boards of Gilead, ViiV, consulting for Merck, Site principal investigator for multisite studies funded by Gilead, Merck, and 1 investigator-initiated study funded by Gilead. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- Tennessee Department of Health . Notification of changes in the HIV program. 2023. Available at: https://wpln.org/wp-content/uploads/sites/7/2023/01/Notification-HIV-Fun.... Accessed 17 July 2023.
-
- Centers for Disease Control and Prevention (CDC) . HIV surveillance report 2020. Center for disease control and prevention. Report No.: Volume 33. Available at: https://www.cdc.gov/hiv/library/reports/hiv-surveillance/vol-33/index.html. Accessed 17 July 2023.
-
- Ahonkhai A, Person A, Pettit A. Where do we go from here: HIV prevention in Tennessee and beyond. IDSA Infectious Diseases Society of America. ; Available at: https://www.idsociety.org/science-speaks-blog/2023/where-do-we-go-from-h.... Accessed 17 July 2023.
-
- amfAR. Statement from amfAR on Tennessee's rejection of federal funds for HIV services. amfAR, The Foundation for AIDS Research. Available at: https://www.amfar.org/news/statement-from-amfar-on-tennessees-rejection-.... Accessed 17 July 2023.
-
- Zuniga JM. IAPAC calls on US congress to reject efforts to gut US HIV response. International Association of Providers of AIDS Care. Available at: https://www.iapac.org/2023/07/14/iapac-calls-on-us-congress-to-reject-ef.... Accessed 17 July 2023.
Publication types
MeSH terms
Grants and funding
- R01 MH134724/MH/NIMH NIH HHS/United States
- P30 AI094189/AI/NIAID NIH HHS/United States
- UL1 TR001863/TR/NCATS NIH HHS/United States
- R01 AI042006/AI/NIAID NIH HHS/United States
- UM2 HD111102/HD/NICHD NIH HHS/United States
- K08 HD094638-05S1/Eunice Kennedy Shriver National Institute for Child Health and Human Development
- P30 AI110527/AI/NIAID NIH HHS/United States
- NH/NIH HHS/United States
- DP2 DA049282/DA/NIDA NIH HHS/United States
- K08 HD094638/HD/NICHD NIH HHS/United States
- R37 DA015612/DA/NIDA NIH HHS/United States
- R01 MD011770/MD/NIMHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
