

Correlation between normally aerated lung and respiratory system compliance at clinical high positive end-expiratory pressure in patients with COVID-19
- PMID: 38914620
- PMCID: PMC11196724
- DOI: 10.1038/s41598-024-64622-3
Correlation between normally aerated lung and respiratory system compliance at clinical high positive end-expiratory pressure in patients with COVID-19
Abstract
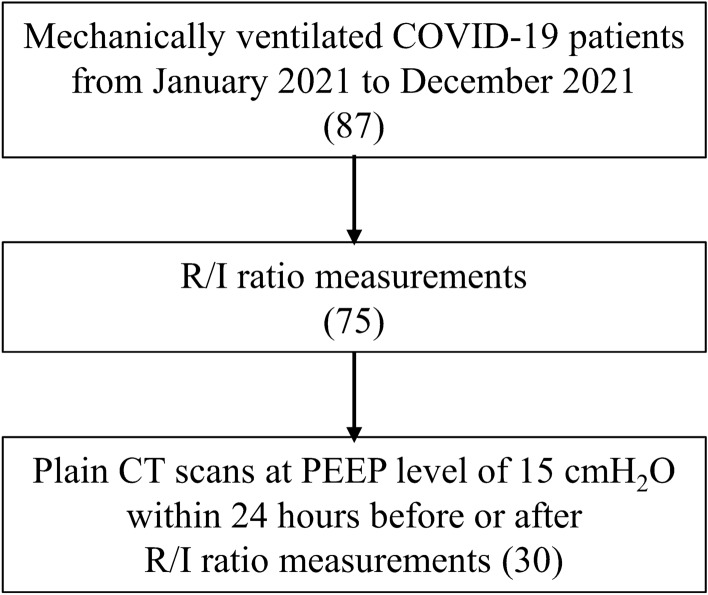
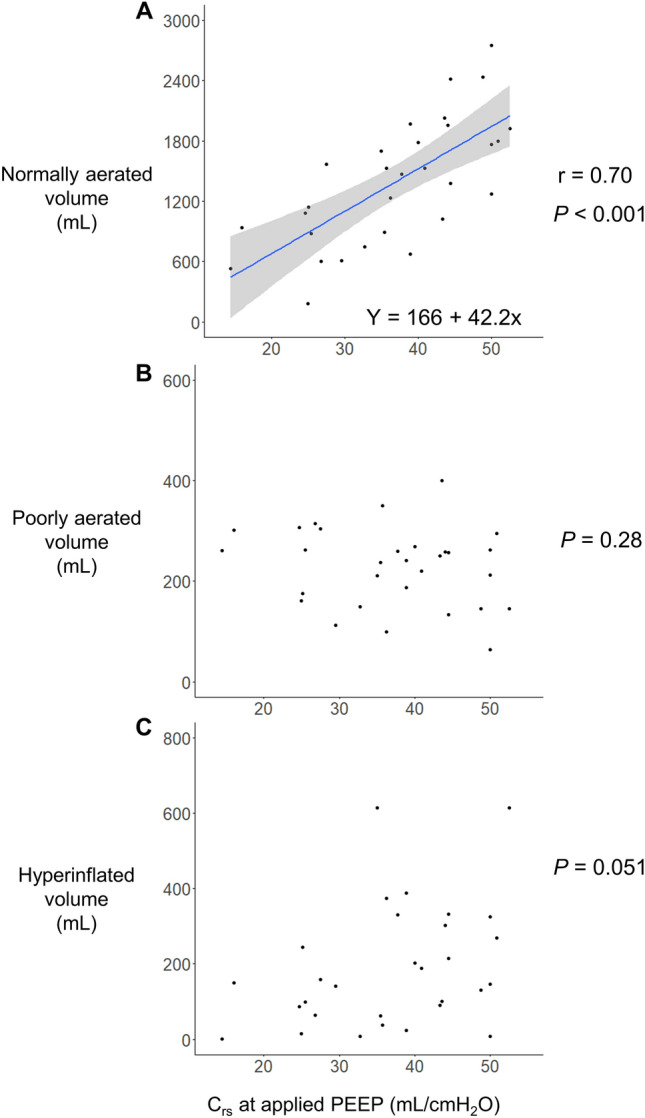
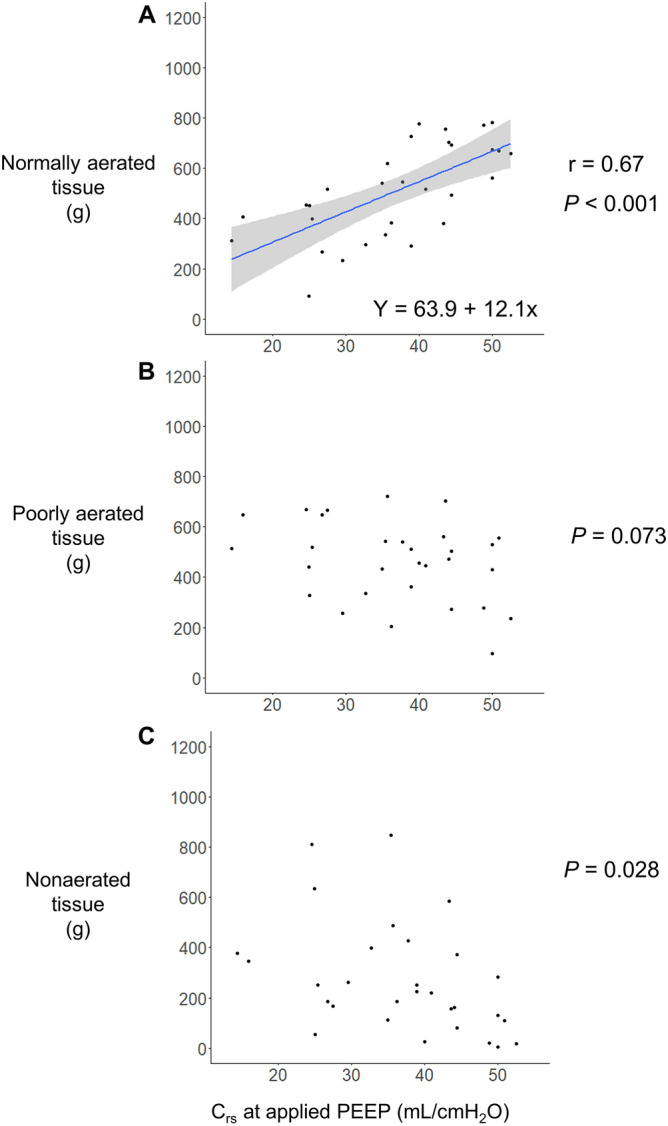
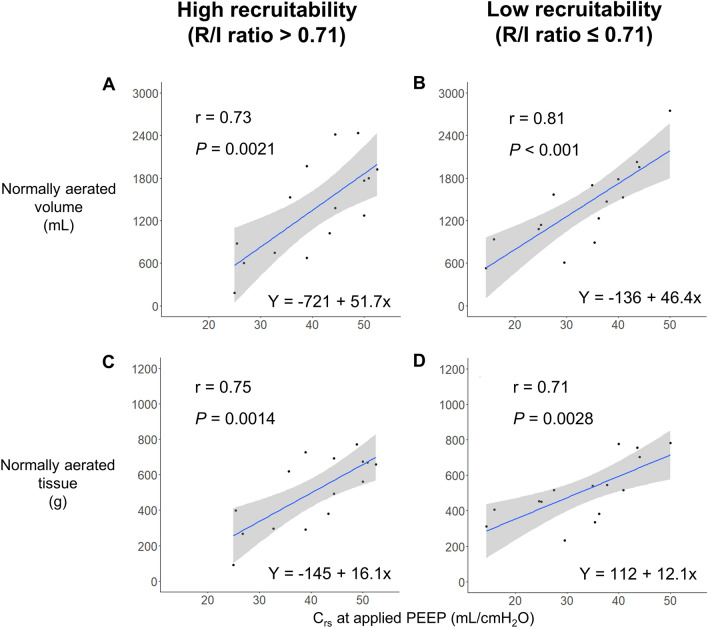
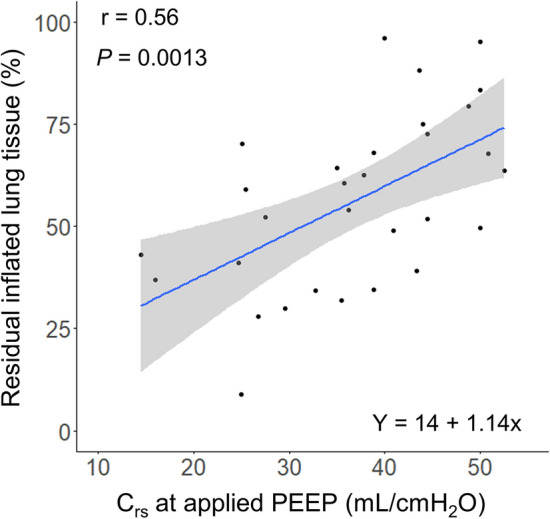
Normally aerated lung tissue on computed tomography (CT) is correlated with static respiratory system compliance (Crs) at zero end-expiratory pressure. In clinical practice, however, patients with acute respiratory failure are often managed using elevated PEEP levels. No study has validated the relationship between lung volume and tissue and Crs at the applied positive end-expiratory pressure (PEEP). Therefore, this study aimed to demonstrate the relationship between lung volume and tissue on CT and Crs during the application of PEEP for the clinical management of patients with acute respiratory distress syndrome due to COVID-19. Additionally, as a secondary outcome, the study aimed to evaluate the relationship between CT characteristics and Crs, considering recruitability using the recruitment-to-inflation ratio (R/I ratio). We analyzed the CT and respiratory mechanics data of 30 patients with COVID-19 who were mechanically ventilated. The CT images were acquired during mechanical ventilation at PEEP level of 15 cmH2O and were quantitatively analyzed using Synapse Vincent system version 6.4 (Fujifilm Corporation, Tokyo, Japan). Recruitability was stratified into two groups, high and low recruitability, based on the median R/I ratio of our study population. Thirty patients were included in the analysis with the median R/I ratio of 0.71. A significant correlation was observed between Crs at the applied PEEP (median 15 [interquartile range (IQR) 12.2, 15.8]) and the normally aerated lung volume (r = 0.70 [95% CI 0.46-0.85], P < 0.001) and tissue (r = 0.70 [95% CI 0.46-0.85], P < 0.001). Multivariable linear regression revealed that recruitability (Coefficient = - 390.9 [95% CI - 725.0 to - 56.8], P = 0.024) and Crs (Coefficient = 48.9 [95% CI 32.6-65.2], P < 0.001) were significantly associated with normally aerated lung volume (R-squared: 0.58). In this study, Crs at the applied PEEP was significantly correlated with normally aerated lung volume and tissue on CT. Moreover, recruitability indicated by the R/I ratio and Crs were significantly associated with the normally aerated lung volume. This research underscores the significance of Crs at the applied PEEP as a bedside-measurable parameter and sheds new light on the link between recruitability and normally aerated lung.
Keywords: Computed tomography; Coronavirus disease 2019; Mechanical ventilation; Recruitability; Respiratory distress syndrome; Respiratory system compliance.
© 2024. The Author(s).
Conflict of interest statement
SK has a contract to consult with Hamilton Medical. The other authors declare no competing interests.
Figures
Similar articles
-
Potential for the lung recruitment and the risk of lung overdistension during 21 days of mechanical ventilation in patients with COVID-19 after noninvasive ventilation failure: the COVID-VENT observational trial.BMC Anesthesiol. 2022 Mar 4;22(1):59. doi: 10.1186/s12871-022-01600-0. BMC Anesthesiol. 2022. PMID: 35246024 Free PMC article.
-
Recruitability and effect of PEEP in SARS-Cov-2-associated acute respiratory distress syndrome.Ann Intensive Care. 2020 May 12;10(1):55. doi: 10.1186/s13613-020-00675-7. Ann Intensive Care. 2020. PMID: 32399901 Free PMC article.
-
How large is the lung recruitability in early acute respiratory distress syndrome: a prospective case series of patients monitored by computed tomography.Crit Care. 2012 Jan 8;16(1):R4. doi: 10.1186/cc10602. Crit Care. 2012. PMID: 22226331 Free PMC article.
-
Recruitment-to-inflation ratio for bedside PEEP selection in acute respiratory distress syndrome.Minerva Anestesiol. 2024 Jul-Aug;90(7-8):694-706. doi: 10.23736/S0375-9393.24.17982-5. Minerva Anestesiol. 2024. PMID: 39021144 Review.
-
Electrical impedance tomography to set positive end-expiratory pressure.Curr Opin Crit Care. 2025 Jun 1;31(3):319-327. doi: 10.1097/MCC.0000000000001255. Epub 2025 Feb 12. Curr Opin Crit Care. 2025. PMID: 39976222 Free PMC article. Review.
