

Deep learning models for predicting the survival of patients with medulloblastoma based on a surveillance, epidemiology, and end results analysis
- PMID: 38914641
- PMCID: PMC11196279
- DOI: 10.1038/s41598-024-65367-9
Deep learning models for predicting the survival of patients with medulloblastoma based on a surveillance, epidemiology, and end results analysis
Abstract
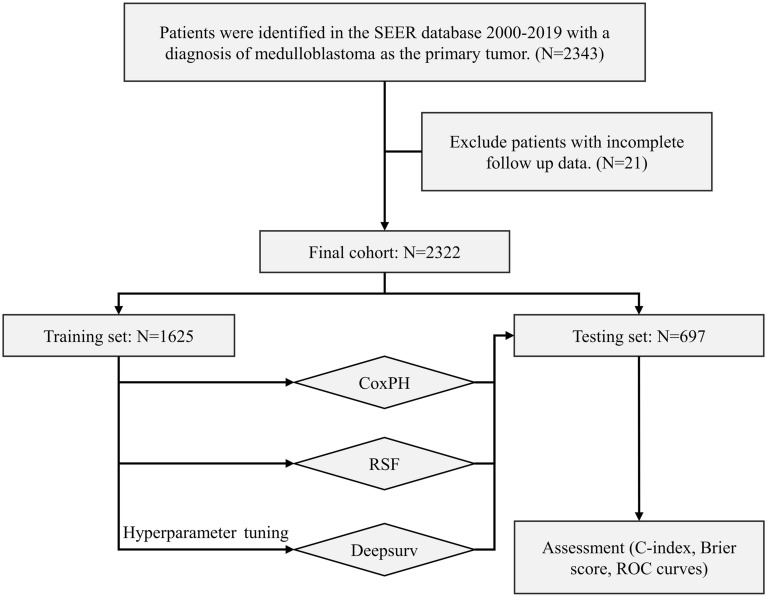
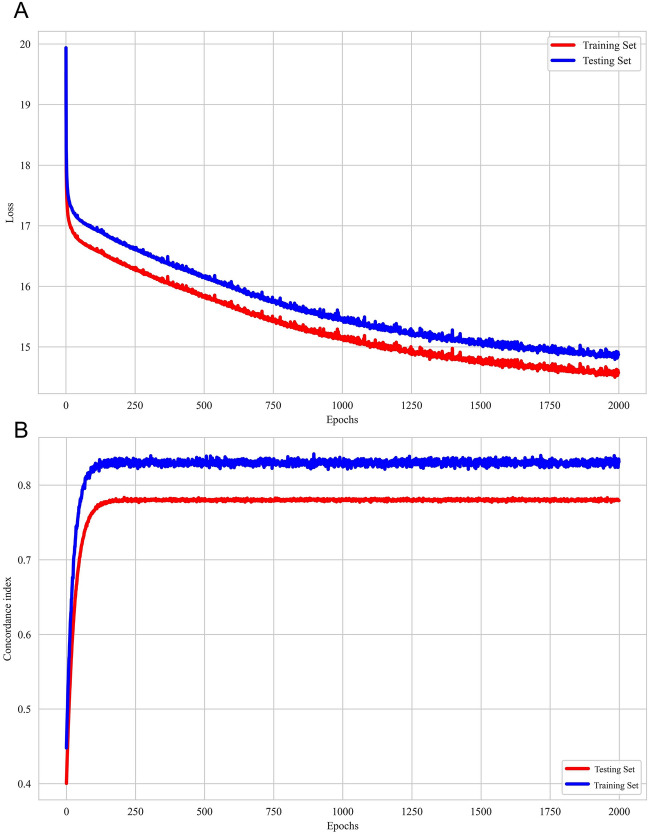
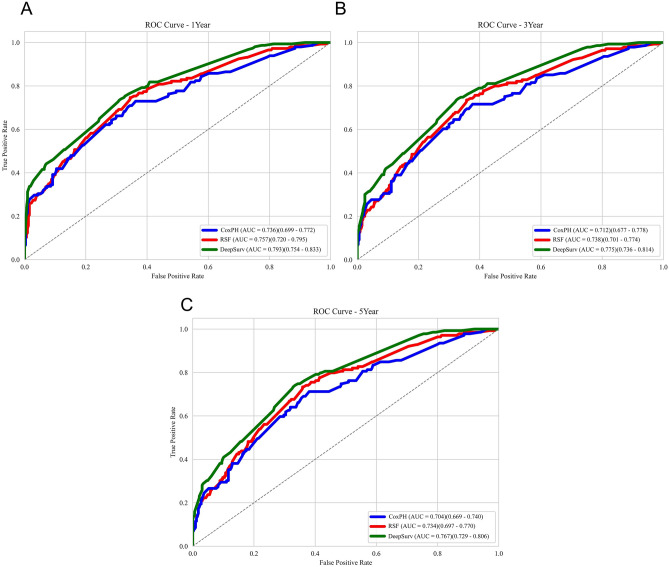
Medulloblastoma is a malignant neuroepithelial tumor of the central nervous system. Accurate prediction of prognosis is essential for therapeutic decisions in medulloblastoma patients. We analyzed data from 2,322 medulloblastoma patients using the SEER database and randomly divided the dataset into training and testing datasets in a 7:3 ratio. We chose three models to build, one based on neural networks (DeepSurv), one based on ensemble learning that Random Survival Forest (RSF), and a typical Cox Proportional-hazards (CoxPH) model. The DeepSurv model outperformed the RSF and classic CoxPH models with C-indexes of 0.751 and 0.763 for the training and test datasets. Additionally, the DeepSurv model showed better accuracy in predicting 1-, 3-, and 5-year survival rates (AUC: 0.767-0.793). Therefore, our prediction model based on deep learning algorithms can more accurately predict the survival rate and survival period of medulloblastoma compared to other models.
Keywords: DeepSurv; Medulloblastoma; Neural network; SEER; Survival prediction.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
