

Altered pupil light and darkness reflex and eye-blink responses in late-life depression
- PMID: 38914987
- PMCID: PMC11194921
- DOI: 10.1186/s12877-024-05034-w
Altered pupil light and darkness reflex and eye-blink responses in late-life depression
Abstract
Background: Late-life depression (LLD) is a prevalent neuropsychiatric disorder in the older population. While LLD exhibits high mortality rates, depressive symptoms in older adults are often masked by physical health conditions. In younger adults, depression is associated with deficits in pupil light reflex and eye blink rate, suggesting the potential use of these responses as biomarkers for LLD.
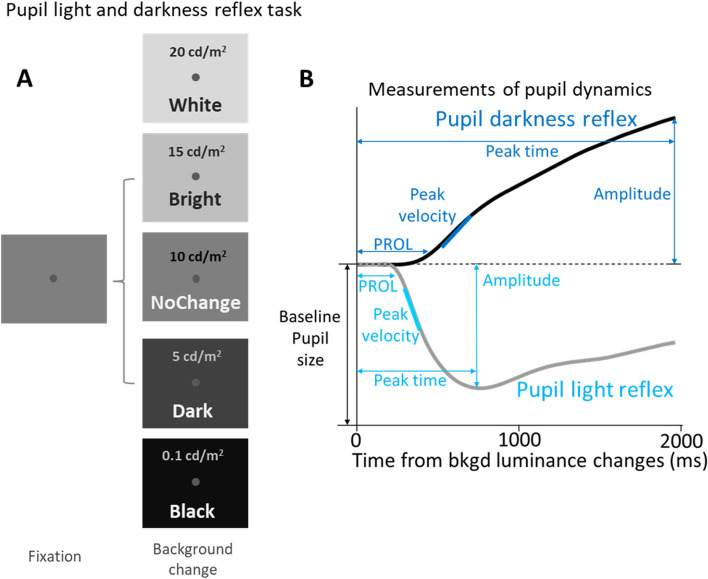
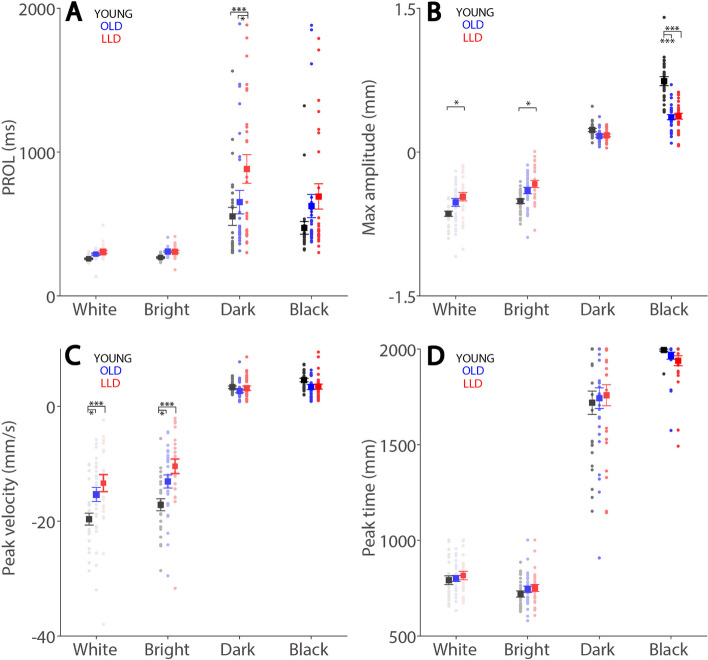
Methods: We conducted a study using video-based eye-tracking to investigate pupil and blink responses in LLD patients (n = 25), older (OLD) healthy controls (n = 29), and younger (YOUNG) healthy controls (n = 25). The aim was to determine whether there were alterations in pupil and blink responses in LLD compared to both OLD and YOUNG groups.
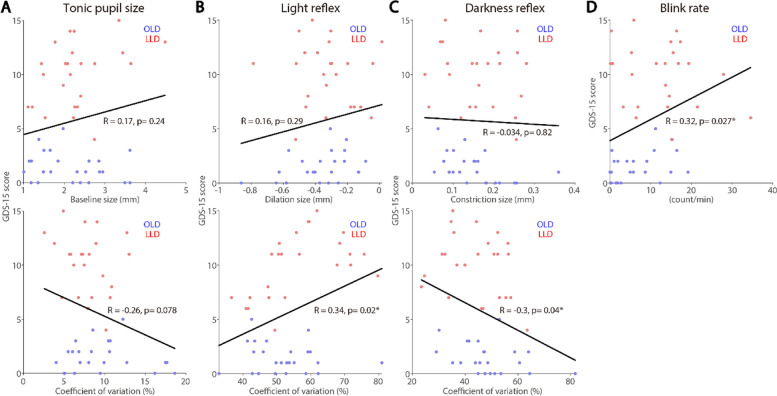
Results: LLD patients displayed significantly higher blink rates and dampened pupil constriction responses compared to OLD and YOUNG controls. While tonic pupil size in YOUNG differed from that of OLD, LLD patients did not exhibit a significant difference compared to OLD and YOUNG controls. GDS-15 scores in older adults correlated with light and darkness reflex response variability and blink rates. PHQ-15 scores showed a correlation with blink rates, while MoCA scores correlated with tonic pupil sizes.
Conclusions: The findings demonstrate that LLD patients display altered pupil and blink behavior compared to OLD and YOUNG controls. These altered responses correlated differently with the severity of depressive, somatic, and cognitive symptoms, indicating their potential as objective biomarkers for LLD.
Keywords: Autonomic function; Eye blink rate; Pupil light and darkness reflex; Pupillometry.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures




References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
