

Impact of sex and socioeconomic status on the likelihood of surgery, hospitalization, and use of medications in inflammatory bowel disease: a systematic review and meta-analysis
- PMID: 38915086
- PMCID: PMC11194997
- DOI: 10.1186/s13643-024-02584-3
Impact of sex and socioeconomic status on the likelihood of surgery, hospitalization, and use of medications in inflammatory bowel disease: a systematic review and meta-analysis
Abstract
Background: Inflammatory bowel diseases (IBDs) are associated with high healthcare utilization. This systematic review aimed to summarize what is known about the impact of sex, income, and education on the likelihood of bowel surgery, hospitalization, and use of corticosteroids and biologics among patients with IBD.
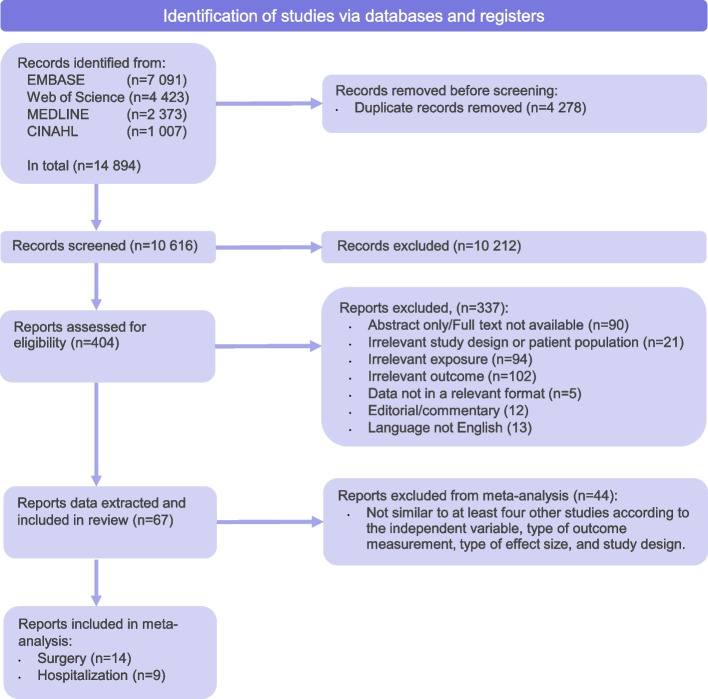
Methods: We used EMBASE, MEDLINE, CINAHL, and Web of Science to perform a systematic literature search. Pooled hazard ratios (HRs) and odds ratios (ORs) with 95% confidence intervals (CIs) were calculated using random effects meta-analysis for the impact of sex on the likelihood of surgery and hospitalization. In addition, we performed subgroup analyses of the effect of IBD type (Crohn's disease or ulcerative colitis) and age. Finally, meta-regression was undertaken for the year of publication.
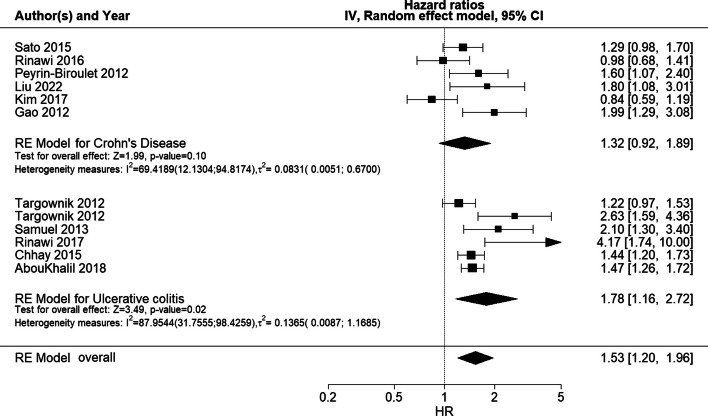
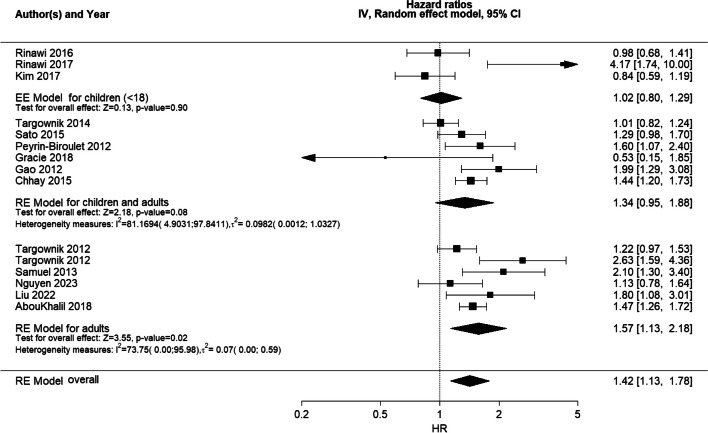
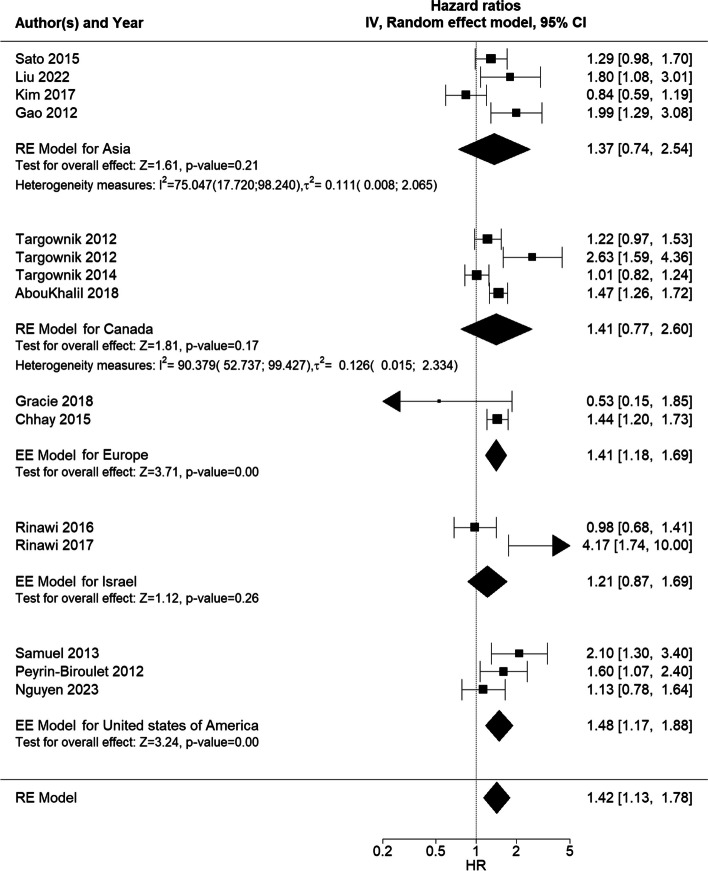
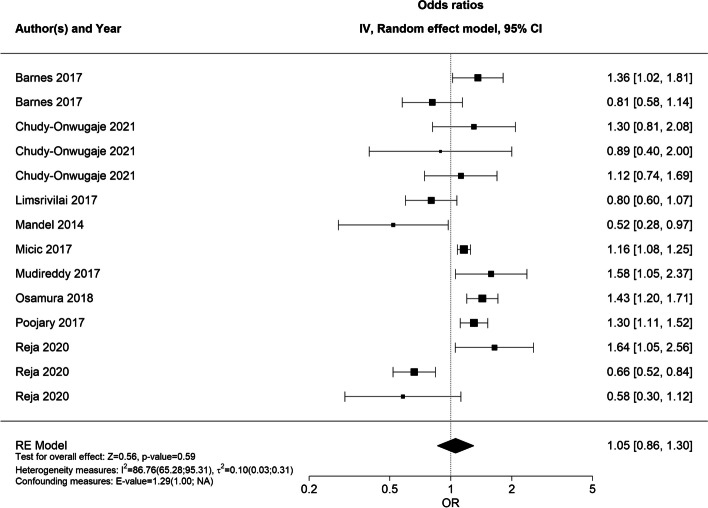
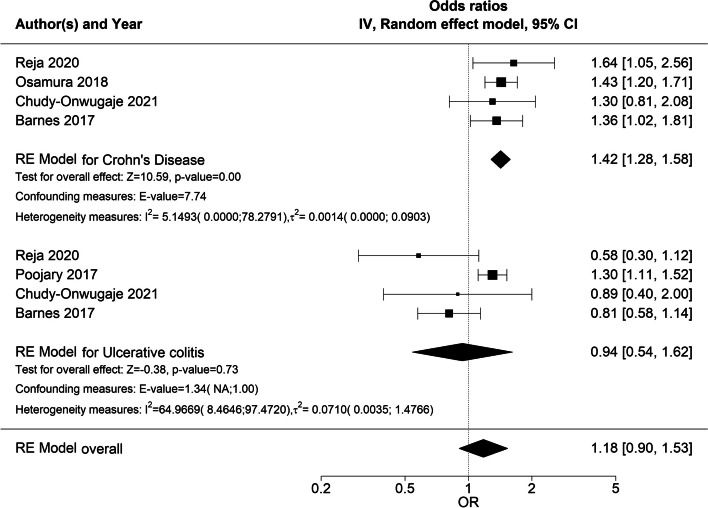
Results: In total, 67 studies were included, of which 23 studies were eligible for meta-analysis. In the main meta-analysis, male sex was associated with an increased likelihood of bowel surgery (HR 1.42 (95% CI 1.13;1.78), which was consistent with the subgroup analysis for UC only (HR 1.78, 95% CI 1.16; 2.72). Sex did not impact the likelihood of hospitalization (OR 1.05 (95% CI 0.86;1.30), although the subgroup analysis revealed an increased likelihood of hospitalization in CD patients (OR 1.42, 95% CI 1.28;1.58). In 9 of 10 studies, no significant sex-based differences in the use of biologics were reported, although in 6 of 6 studies, female patients had lower adherence to biologics. In 11 of 13 studies, no significant sex-based difference in the use of corticosteroids was reported. The evidence of the impact of income and education on healthcare utilization was sparse and pointed in different directions. The substantial heterogeneity between studies was explained, in part, by differences in IBD type and age.
Conclusions: The results of this systematic review indicate that male patients with IBD are significantly more likely to have surgery than female patients with IBD but are not, overall, more likely to be hospitalized, whereas female patients appear to have statistically significantly lower adherence to biologics compared to male patients. Thus, clinicians should not underestimate the impact of sex on healthcare utilization. Evidence for income- and education-based differences remains sparse.
Systematic review registration: PROSPERO CRD42022315788.
Keywords: Hospitalization; Inflammatory bowel disease; Sex differences; Socioeconomic differences; Surgery.
© 2024. The Author(s).
Conflict of interest statement
TJ reports consulting for Ferring and Pfizer. All other authors declare that they have no competing interests.
Figures

Similar articles
-
Sex-related differences in profiles and clinical outcomes of Inflammatory bowel disease: a systematic review and meta-analysis.BMC Gastroenterol. 2024 Nov 23;24(1):425. doi: 10.1186/s12876-024-03514-2. BMC Gastroenterol. 2024. PMID: 39580396 Free PMC article.
-
Systematic Review and Meta-Analysis: Risk of Hospitalization in Patients with Ulcerative Colitis and Crohn's Disease in Population-Based Cohort Studies.Dig Dis Sci. 2022 Jun;67(6):2451-2461. doi: 10.1007/s10620-021-07200-1. Epub 2021 Aug 11. Dig Dis Sci. 2022. PMID: 34379220 Free PMC article.
-
Impact of Low Immunoglobulin G Levels on Disease Outcomes in Patients with Inflammatory Bowel Diseases.Dig Dis Sci. 2016 Nov;61(11):3270-3277. doi: 10.1007/s10620-016-4294-z. Epub 2016 Sep 12. Dig Dis Sci. 2016. PMID: 27619393
-
Risk of postoperative infectious complications from medical therapies in inflammatory bowel disease.Cochrane Database Syst Rev. 2020 Oct 24;10(10):CD013256. doi: 10.1002/14651858.CD013256.pub2. Cochrane Database Syst Rev. 2020. PMID: 33098570 Free PMC article.
-
Significant Racial and Ethnic Disparities Exist in Health Care Utilization in Inflammatory Bowel Disease: A Systematic Review and Meta-analysis.Inflamm Bowel Dis. 2024 Mar 1;30(3):470-481. doi: 10.1093/ibd/izad045. Inflamm Bowel Dis. 2024. PMID: 36975373
Cited by
-
[An update on surgical treatment options for inflammatory bowel disease].Inn Med (Heidelb). 2025 Feb;66(2):174-180. doi: 10.1007/s00108-024-01846-5. Epub 2025 Jan 30. Inn Med (Heidelb). 2025. PMID: 39883175 Free PMC article. Review. German.
-
Sex-Based Disparities in Treatment and Healthcare Utilization in Patients with Ulcerative Colitis: A Systematic Review and Meta-Analysis.J Clin Med. 2024 Dec 11;13(24):7534. doi: 10.3390/jcm13247534. J Clin Med. 2024. PMID: 39768465 Free PMC article. Review.
References
-
- Burisch J, Vardi H, Schwartz D, Friger M, Kiudelis G, Kupčinskas J, et al. Health-care costs of inflammatory bowel disease in a pan-European, community-based, inception cohort during 5 years of follow-up: a population-based study. Lancet Gastroenterol Hepatol. 2020;5(5):454–464. doi: 10.1016/S2468-1253(20)30012-1. - DOI - PubMed
-
- Alatab S, Sepanlou SG, Ikuta K, Vahedi H, Bisignano C, Safiri S, et al. The global, regional, and national burden of inflammatory bowel disease in 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol Hepatol. 2020;5(1):17–30. doi: 10.1016/S2468-1253(19)30333-4. - DOI - PMC - PubMed
-
- Zhao M, Sall Jensen M, Knudsen T, Kelsen J, Coskun M, Kjellberg J, et al. Trends in the use of biologicals and their treatment outcomes among patients with inflammatory bowel diseases – a Danish nationwide cohort study. Aliment Pharmacol Ther. 2022;55(5):541–557. doi: 10.1111/apt.16723. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
