

Stringent monitoring can decrease mortality of immune checkpoint inhibitor induced cardiotoxicity
- PMID: 38915743
- PMCID: PMC11194425
- DOI: 10.3389/fcvm.2024.1408586
Stringent monitoring can decrease mortality of immune checkpoint inhibitor induced cardiotoxicity
Abstract
Background: Immune checkpoint inhibitor (ICI)-induced myocarditis is a rare immune-related adverse event (irAE) with a fatality rate of 40%-46%. However, irMyocarditis can be asymptomatic. Thus, improved monitoring, detection and therapy are needed. This study aims to generate knowledge on pathogenesis and assess outcomes in cancer centers with intensified patient management.
Methods: Patients with cardiac irAEs from the SERIO registry (www.serio-registry.org) were analyzed for demographics, ICI-related information (type of ICI, therapy line, combination with other drugs, onset of irAE, and tumor response), examination results, irAE treatment and outcome, as well as oncological endpoints. Cardiac biopsies of irMyocarditis cases (n = 12) were analyzed by Nanostring and compared to healthy heart muscle (n = 5) and longitudinal blood sampling was performed for immunophenotyping of irMyocarditis-patients (n = 4 baseline and n = 8 during irAE) in comparison to patients without toxicity under ICI-therapy (n = 4 baseline and n = 7 during ICI-therapy) using flow cytometry.
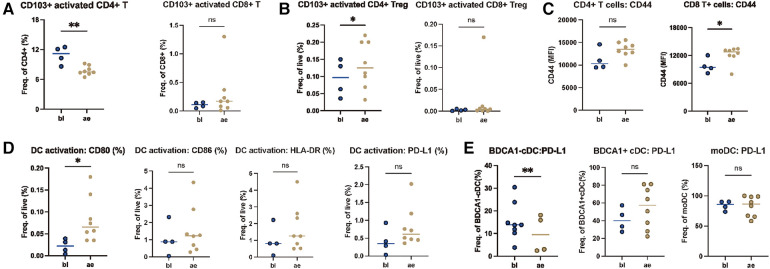
Results: A total of 51 patients with 53 cardiac irAEs induced by 4 different ICIs (anti-PD1, anti-PD-L1, anti-CTLA4) were included from 12 centers in 3 countries. Altogether, 83.0% of cardiac irAEs were graded as severe or life-threatening, and 11.3% were fatal (6/53). Thus, in centers with established consequent troponin monitoring, work-up upon the rise in troponin and consequent treatment of irMyocarditis with corticosteroids and -if required-second-line therapy mortality rate is much lower than previously reported. The median time to irMyocarditis was 36 days (range 4-1,074 days) after ICI initiation, whereas other cardiotoxicities, e.g. asystolia or myocardiopathy, occurred much later. The cytokine-mediated signaling pathway was differentially regulated in myocardial biopsies as compared to healthy heart based on enrichment Gene Ontology analysis. Additionally, longitudinal peripheral blood mononuclear cell (PBMC) samples from irMyocarditis-patients indicated ICI-driven enhanced CD4+ Treg cells and reduced CD4+ T cells. Immunophenotypes, particularly effector memory T cells of irMyocarditis-patients differed from those of ICI-treated patients without side effects. LAG3 expression on T cells and PD-L1 expression on dendritic cells could serve as predictive indicators for the development of irMyocarditis.
Conclusion: Interestingly, our cohort shows a very low mortality rate of irMyocarditis-patients. Our data indicate so far unknown local and systemic immunological patterns in cardiotoxicity.
Keywords: cardiovascular toxicity; checkpoint inhibitor; immunotherapy; melanoma; myocarditis.
© 2024 Wang, Ertl, Schmitt, Hammann, Kramer, Grabmaier, Schöberl, Anz, Piseddu, Pesch, Vera, Froehlich, Weckbach, Tomsitz, Loquai, Zimmer, Mangana, Dummer, Gutzmer, Klespe, Stege, Meiss, Thoms, Terheyden, Bröckelmann, Johnson, French and Heinzerling.
Conflict of interest statement
LH received speaker and consultancy fees from BiomeDx, BMS, Immunocore, Kyowa Kirin, Merck, MSD, Myoncare, Novartis, Pieris, Pierre-Fabre, Roche, Sanofi, Stemline Therapeutics, SUN and Therakos. The LMU received research grants or clinical study grants from Agenus, AstraZeneca Inc., BMS, Hoffmann-La Roche AG, Huya Bioscience, Immunocore, IO Biotech, Merck, Merck Sharp & Dome GmbH, Miltenyi Biomedicine GmbH, Novartis, Pfizer, Pierre Fabre, Regeneron, Replimune, and Sanofi Aventis. CE reports on speaker fees from BristolMyers Squibb, GSK, Immunocore, Kyowa Kirin, MSD CL received honoraria (lectures, presentations, speakers bureaus, manuscript writing or educational events) and travel support from: BMS, MSD Merck, Pierre-Fabre, Biontech, Almirall Hermal, Sun Pharma, KyowaKirin, Immunocore, Sanofi, Novartis. DT reports consultancy, speaker fees or travel grants: BMS, Roche, Novartis, Sanofi, Recordati, Kyowa Kirin, Sun Pharma and Pierre Fabre. LZ served as consultant and has received honoraria from BMS, MSD, Novartis, Pierre Fabre, Sanofi, and Sunpharma and travel support from MSD, BMS, Pierre Fabre, Sanofi, Sunpharma and Novartis, outside the submitted work. PJB reports research funding (inst) by BeiGene, BMS, MSD and Takeda; an advisory role to BeiGene, BMS, MSD, Need Inc., Stemline and Takeda; honoraria from BeiGene, BMS, Celgene, MSD, Need Inc., Stemline and Takeda and stock options from Need Inc. RG received honoraria for advice and lectures from BristolMyers Squibb, Roche Pharma, MerckSharpDohme, Novartis, Merck-Serono, Amgen, Almirall Hermal, Pierre-Fabre, Sun Pharma, Immunocore, 4SC, Delcath, Sanofi/Regeneron. Ralf Gutzmer received travel support from SUN Pharma, Boehringer Ingelheim and PierreFabre. Ralf Gutzmer received research grants from Novartis, Sanofi/Regeneron, Merck Serono, Amgen, SUN Pharma, KyowaKirin, Admiral Hermal. RD has intermittent, project focused consulting and/or advisory relationships with Novartis, Merck Sharp & Dhome (MSD), Bristol-Myers Squibb (BMS), Roche, Amgen, Takeda, Pierre Fabre, Sun Pharma, Sanofi, Catalym, Second Genome, Regeneron, Alligator, T3 Pharma, MaxiVAX SA, Pfizer, Simcere and touchIME outside the submitted work. All remaining authors have declared no conflicts of interest. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures




References
LinkOut - more resources
Full Text Sources
Research Materials