

No Effect of Methylnaltrexone on Acute Pancreatitis Severity: A Multicenter Randomized Controlled Trial
- PMID: 38916223
- PMCID: PMC11524628
- DOI: 10.14309/ajg.0000000000002904
No Effect of Methylnaltrexone on Acute Pancreatitis Severity: A Multicenter Randomized Controlled Trial
Abstract
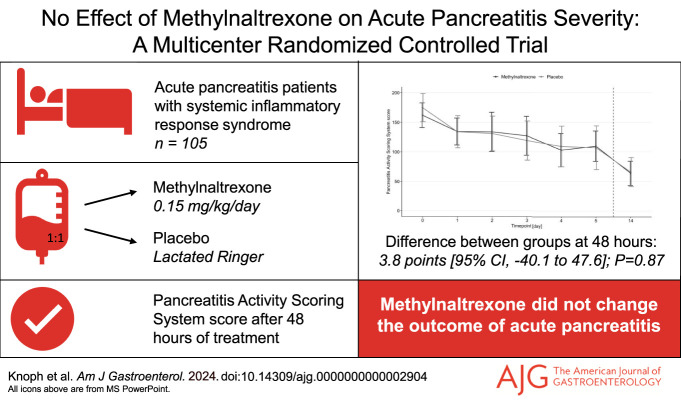
Introduction: Opioids used to manage severe pain in acute pancreatitis (AP) might exacerbate the disease through effects on gastrointestinal and immune functions. Methylnaltrexone, a peripherally acting µ-opioid receptor antagonist, may counteract these effects without changing analgesia.
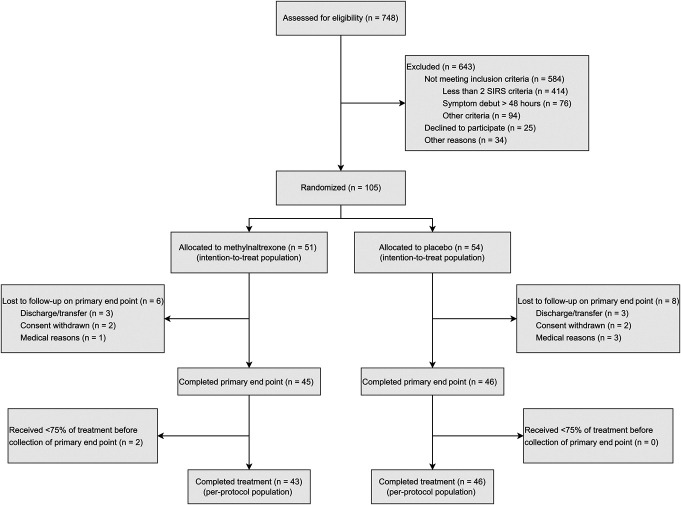
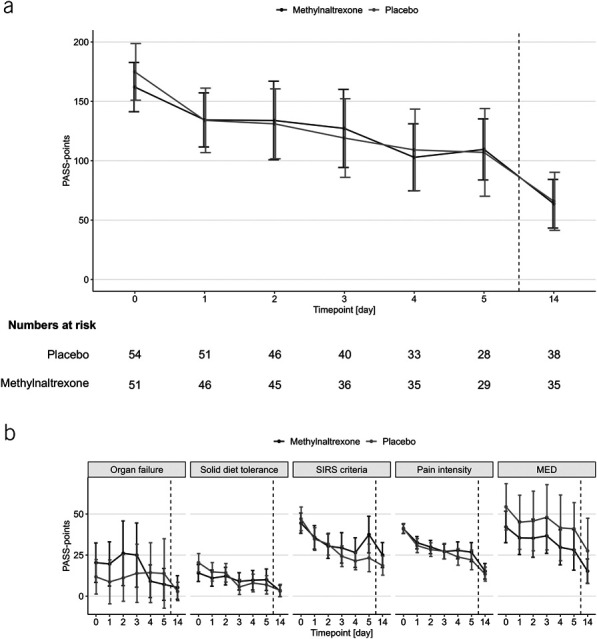
Methods: This double-blind, randomized, placebo-controlled trial included adult patients with AP and systemic inflammatory response syndrome at 4 Danish centers. Patients were randomized to receive 5 days of continuous intravenous methylnaltrexone (0.15 mg/kg/d) or placebo added to the standard of care. The primary end point was the Pancreatitis Activity Scoring System score after 48 hours of treatment. Main secondary outcomes included pain scores, opioid use, disease severity, and mortality.
Results: In total, 105 patients (54% men) were randomized to methylnaltrexone (n = 51) or placebo (n = 54). After 48 hours, the Pancreatitis Activity Scoring System score was 134.3 points in the methylnaltrexone group and 130.5 points in the placebo group (difference 3.8, 95% confidence interval [CI] -40.1 to 47.6; P = 0.87). At 48 hours, we found no differences between the groups in pain severity (0.0, 95% CI -0.8 to 0.9; P = 0.94), pain interference (-0.3, 95% CI -1.4 to 0.8; P = 0.55), and morphine equivalent doses (6.5 mg, 95% CI -2.1 to 15.2; P = 0.14). Methylnaltrexone also did not affect the risk of severe disease (8%, 95% CI -11 to 28; P = 0.38) and mortality (6%, 95% CI -1 to 12; P = 0.11). The medication was well tolerated.
Discussion: Methylnaltrexone treatment did not achieve superiority over placebo for reducing the severity of AP.
Trial registration: ClinicalTrials.gov NCT04743570.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of The American College of Gastroenterology.
Conflict of interest statement
Figures
References
-
- Iannuzzi JP, King JA, Leong JH, et al. . Global incidence of acute pancreatitis is increasing over time: A systematic review and meta-analysis. Gastroenterology 2022;162(1):122–34. - PubMed
-
- Banks PA, Bollen TL, Dervenis C, et al. . Classification of acute pancreatitis--2012: Revision of the Atlanta classification and definitions by international consensus. Gut 2013;62(1):102–11. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
