

In vitro identification of underutilized β-lactam combinations against methicillin-resistant Staphylococcus aureus bacteremia isolates
- PMID: 38916355
- PMCID: PMC11302340
- DOI: 10.1128/spectrum.00976-24
In vitro identification of underutilized β-lactam combinations against methicillin-resistant Staphylococcus aureus bacteremia isolates
Abstract
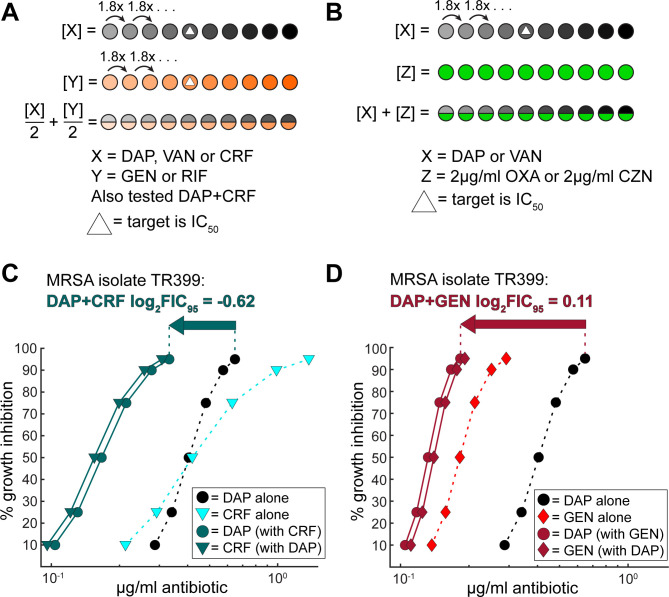
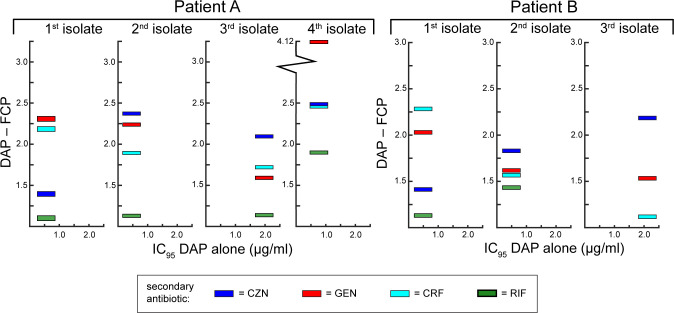
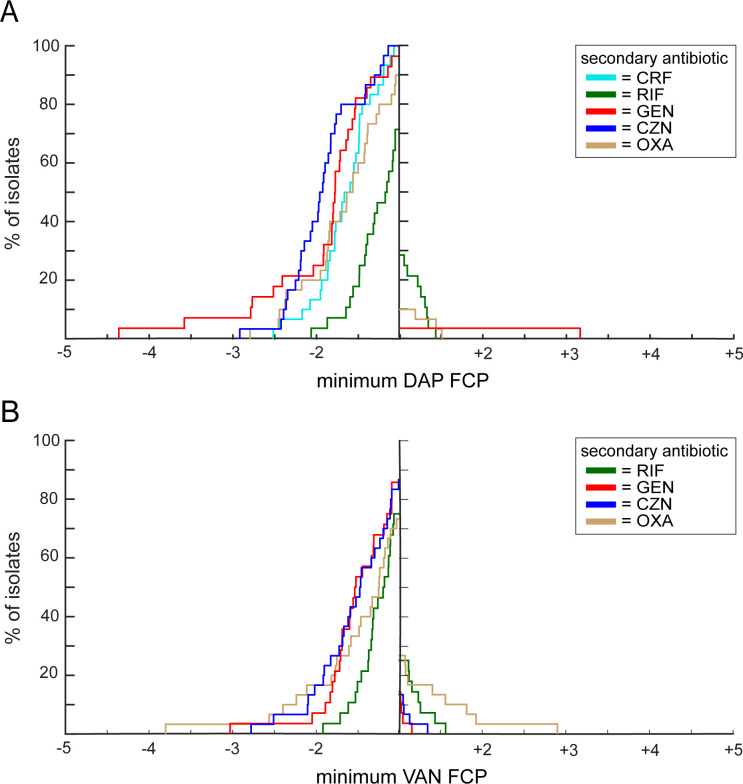
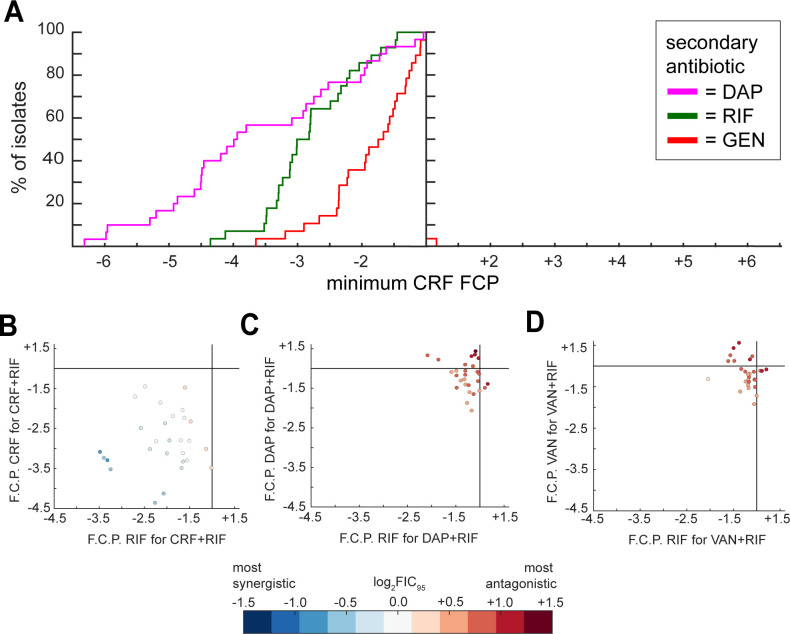
Methicillin-resistant Staphylococcus aureus (MRSA) bacteremia is a serious clinical challenge with high mortality rates. Antibiotic combination therapy is currently used in cases of persistent infection; however, the limited development of new antibiotics will likely increase the need for combination therapy, and better methods are needed for identifying effective combinations for treating persistent bacteremia. To identify pairwise combinations with the most consistent potential for benefit compared to monotherapy with a primary anti-MRSA agent, we conducted a systematic study with an in vitro high-throughput methodology. We tested daptomycin and vancomycin each in combination with gentamicin, rifampicin, cefazolin, and oxacillin, and ceftaroline with daptomycin, gentamicin, and rifampicin. Combining cefazolin with daptomycin lowered the daptomycin concentration required to reach 95% growth inhibition (IC95) for all isolates tested and lowered daptomycin IC95 below the sensitivity breakpoint for five out of six isolates that had daptomycin minimum inhibitory concentrations at or above the sensitivity breakpoint. Similarly, vancomycin IC95s were decreased when vancomycin was combined with cefazolin for 86.7% of the isolates tested. This was a higher percentage than was achieved by adding any other secondary antibiotic to vancomycin. Adding rifampicin to daptomycin or vancomycin did not always reduce IC95s and failed to produce synergistic interaction in any of the isolates tested; the addition of rifampicin to ceftaroline was frequently synergistic and always lowered the amount of ceftaroline required to reach the IC95. These analyses rationalize further in vivo evaluation of three drug pairs for MRSA bacteremia: daptomycin+cefazolin, vancomycin+cefazolin, and ceftaroline+rifampicin.IMPORTANCEBloodstream infections caused by methicillin-resistant Staphylococcus aureus (MRSA) have a high mortality rate despite the availability of vancomycin, daptomycin, and newer antibiotics including ceftaroline. With the slow output of the antibiotic pipeline and the serious clinical challenge posed by persistent MRSA infections, better strategies for utilizing combination therapy are becoming increasingly necessary. We demonstrated the value of a systematic high-throughput approach, adapted from prior work testing antibiotic combinations against tuberculosis and other mycobacteria, by using this approach to test antibiotic pairs against a panel of MRSA isolates with diverse patterns of antibiotic susceptibility. We identified three antibiotic pairs-daptomycin+cefazolin, vancomycin+cefazolin, and ceftaroline+rifampicin-where the addition of the second antibiotic improved the potency of the first antibiotic across all or most isolates tested. Our results indicate that these pairs warrant further evaluation in the clinical setting.
Keywords: MRSA; bacteremia; cefazolin; ceftaroline; combination therapy; rifampicin.
Conflict of interest statement
D.R.S. has research contracts with Tufts Medical Center from Prolacta, Summit Therapeutics, Seres Health, and Merck. He is a consultant to Merck, Prolacta, and Seres Health. K.P.D., B.B.A., and L.A.M. have no conflicts of interest to disclose.
Figures
Similar articles
-
Oritavancin Combinations with β-Lactams against Multidrug-Resistant Staphylococcus aureus and Vancomycin-Resistant Enterococci.Antimicrob Agents Chemother. 2016 Mar 25;60(4):2352-8. doi: 10.1128/AAC.03006-15. Print 2016 Apr. Antimicrob Agents Chemother. 2016. PMID: 26833159 Free PMC article.
-
Bacteremia due to Methicillin-Resistant Staphylococcus aureus: An Update on New Therapeutic Approaches.Infect Dis Clin North Am. 2020 Dec;34(4):849-861. doi: 10.1016/j.idc.2020.04.003. Epub 2020 Sep 30. Infect Dis Clin North Am. 2020. PMID: 33011050 Review.
-
In vitro activity of fosfomycin alone and in combination against Staphylococcus aureus with reduced susceptibility or resistance to methicillin, vancomycin, daptomycin or linezolid.J Antimicrob Chemother. 2022 Dec 23;78(1):238-241. doi: 10.1093/jac/dkac380. J Antimicrob Chemother. 2022. PMID: 36374572
-
Genomic investigation and clinical correlates of the in vitro β-lactam: NaHCO3 responsiveness phenotype among methicillin-resistant Staphylococcus aureus isolates from a randomized clinical trial.Antimicrob Agents Chemother. 2024 Jul 9;68(7):e0021824. doi: 10.1128/aac.00218-24. Epub 2024 Jun 5. Antimicrob Agents Chemother. 2024. PMID: 38837393 Free PMC article. Clinical Trial.
-
Vancomycin or Daptomycin Plus a β-Lactam Versus Vancomycin or Daptomycin Alone for Methicillin-Resistant Staphylococcus aureus Bloodstream Infections: A Systematic Review and Meta-Analysis.Microb Drug Resist. 2021 Aug;27(8):1044-1056. doi: 10.1089/mdr.2020.0350. Epub 2021 Mar 15. Microb Drug Resist. 2021. PMID: 33728980
Cited by
-
Adjunctive β-lactams for Staphylococcus aureus bacteremia: a narrative review.Ther Adv Infect Dis. 2025 Jun 14;12:20499361251343969. doi: 10.1177/20499361251343969. eCollection 2025 Jan-Dec. Ther Adv Infect Dis. 2025. PMID: 40529959 Free PMC article. Review.
References
-
- Doernberg SB, Lodise TP, Thaden JT, Munita JM, Cosgrove SE, Arias CA, Boucher HW, Corey GR, Lowy FD, Murray B, Miller LG, Holland TL, Gram-Positive Committee of the Antibacterial Resistance Leadership Group (ARLG) . 2017. Gram-positive bacterial infections: research priorities, accomplishments, and future directions of the antibacterial resistance leadership group. Clin Infect Dis 64:S24–S29. doi:10.1093/cid/ciw828 - DOI - PMC - PubMed
-
- Jernigan JA, Hatfield KM, Wolford H, Nelson RE, Olubajo B, Reddy SC, McCarthy N, Paul P, McDonald LC, Kallen A, Fiore A, Craig M, Baggs J. 2020. Multidrug-resistant bacterial infections in U.S. hospitalized patients, 2012-2017. N Engl J Med 382:1309–1319. doi:10.1056/NEJMoa1914433 - DOI - PMC - PubMed
-
- Liu C, Bayer A, Cosgrove SE, Daum RS, Fridkin SK, Gorwitz RJ, Kaplan SL, Karchmer AW, Levine DP, Murray BE, J. Rybak M, Talan DA, Chambers HF. 2011. Clinical practice guidelines by the infectious diseases society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children: executive summary. Clin Infect Dis 52:285–292. doi:10.1093/cid/cir034 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
