

Biologic and Clinical Analysis of Childhood Gamma Delta T-ALL Identifies LMO2/STAG2 Rearrangements as Extremely High Risk
- PMID: 38916500
- PMCID: PMC11452281
- DOI: 10.1158/2159-8290.CD-23-1452
Biologic and Clinical Analysis of Childhood Gamma Delta T-ALL Identifies LMO2/STAG2 Rearrangements as Extremely High Risk
Abstract
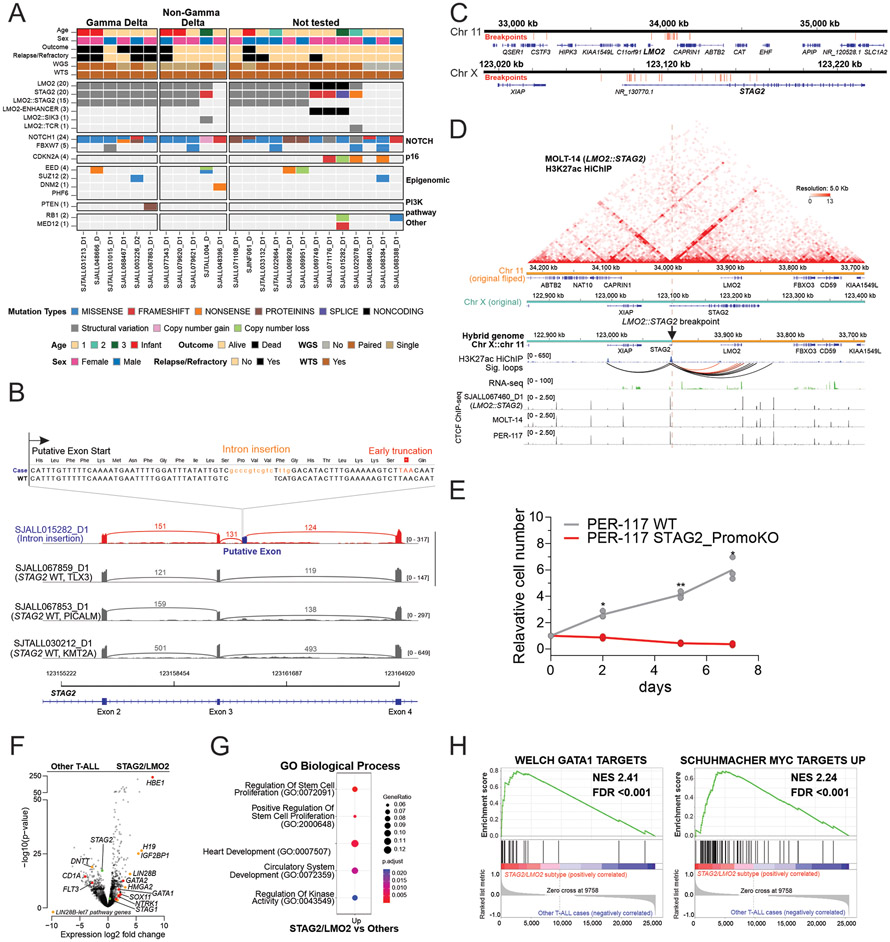
Acute lymphoblastic leukemia expressing the gamma delta T-cell receptor (γδ T-ALL) is a poorly understood disease. We studied 200 children with γδ T-ALL from 13 clinical study groups to understand the clinical and genetic features of this disease. We found age and genetic drivers were significantly associated with outcome. γδ T-ALL diagnosed in children under 3 years of age was extremely high-risk and enriched for genetic alterations that result in both LMO2 activation and STAG2 inactivation. Mechanistically, using patient samples and isogenic cell lines, we show that inactivation of STAG2 profoundly perturbs chromatin organization by altering enhancer-promoter looping, resulting in deregulation of gene expression associated with T-cell differentiation. High-throughput drug screening identified a vulnerability in DNA repair pathways arising from STAG2 inactivation, which can be targeted by poly(ADP-ribose) polymerase inhibition. These data provide a diagnostic framework for classification and risk stratification of pediatric γδ T-ALL. Significance: Patients with acute lymphoblastic leukemia expressing the gamma delta T-cell receptor under 3 years old or measurable residual disease ≥1% at end of induction showed dismal outcomes and should be classified as having high-risk disease. The STAG2/LMO2 subtype was enriched in this very young age group. STAG2 inactivation may perturb chromatin conformation and cell differentiation and confer vulnerability to poly(ADP-ribose) polymerase inhibition.
©2024 American Association for Cancer Research.
Conflict of interest statement
Conflict of interests
D.T.T. received research funding from BEAM Therapeutics, NeoImmune Tech and serves on advisory boards for BEAM Therapeutics, Janssen, Servier, Sobi, and Jazz. D.T.T. has multiple patents pending on CAR-T. I.I. reported consultation honorarium from Arima and travel expenses paid by Mission Bio. M.Kicinski received research funding from MSD, BMS, Pierre Fabre, JnJ, and Immunocore. C.G.M. received research funding from Loxo Oncology, Pfizer, AbbVie; honoraria from Amgen and Illumina, and holds stock in Amgen. There are no conflicts of interest with the work presented in this manuscript.
Figures





References
-
- Winter SS, Dunsmore KP, Devidas M, Wood BL, Esiashvili N, Chen Z, et al. Improved Survival for Children and Young Adults With T-Lineage Acute Lymphoblastic Leukemia: Results From the Children's Oncology Group AALL0434 Methotrexate Randomization. J Clin Oncol 2018;36(29):2926–34 doi 10.1200/JCO.2018.77.7250. - DOI - PMC - PubMed
-
- Dunsmore KP, Winter SS, Devidas M, Wood BL, Esiashvili N, Chen Z, et al. Children's Oncology Group AALL0434: A Phase III Randomized Clinical Trial Testing Nelarabine in Newly Diagnosed T-Cell Acute Lymphoblastic Leukemia. J Clin Oncol 2020;38(28):3282–93 doi 10.1200/JCO.20.00256. - DOI - PMC - PubMed
-
- Sato A, Hatta Y, Imai C, Oshima K, Okamoto Y, Deguchi T, et al. Nelarabine, intensive L-asparaginase, and protracted intrathecal therapy for newly diagnosed T-cell acute lymphoblastic leukaemia in children and young adults (ALL-T11): a nationwide, multicenter, phase 2 trial including randomisation in the very high-risk group. Lancet Haematol 2023;10(6):e419–e32 doi 10.1016/S2352-3026(23)00072-8. - DOI - PubMed
MeSH terms
Substances
Grants and funding
- U24 CA196173/CA/NCI NIH HHS/United States
- K99 CA279756/CA/NCI NIH HHS/United States
- P30 CA021765/CA/NCI NIH HHS/United States
- F32 CA254140/CA/NCI NIH HHS/United States
- U10 CA180820/CA/NCI NIH HHS/United States
- U10 CA180899/CA/NCI NIH HHS/United States
- UNCE/24/MED/003/Charles University Research Center
- U10 CA180866/CA/NCI NIH HHS/United States
- NU23J-03-00026/Ministry of Health of the Czech Republic
- R35 CA197695/CA/NCI NIH HHS/United States
- Henry Schueler 41&9 Foundation
- UG1 CA189859/CA/NCI NIH HHS/United States
- R03 CA256550/CA/NCI NIH HHS/United States
- U24 CA114766/CA/NCI NIH HHS/United States
- X01 HD100702/Common Fund (NIH Common Fund)
- Robert J. Arceci Innovation Award/St. Baldrick's Foundation (SBF)
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
