

Clinical Subphenotypes of Staphylococcus aureus Bacteremia
- PMID: 38916975
- PMCID: PMC11581694
- DOI: 10.1093/cid/ciae338
Clinical Subphenotypes of Staphylococcus aureus Bacteremia
Abstract
Background: Staphylococcus aureus bacteremia (SAB) is a clinically heterogeneous disease. The ability to identify subgroups of patients with shared traits (subphenotypes) is an unmet need to allow patient stratification for clinical management and research. We aimed to test the hypothesis that clinically relevant subphenotypes can be reproducibly identified among patients with SAB.
Methods: We studied 3 cohorts of adults with monomicrobial SAB: a UK retrospective observational study (Edinburgh cohort, n = 458), the UK ARREST trial (n = 758), and the Spanish SAFO trial (n = 214). Latent class analysis was used to identify subphenotypes using routinely collected clinical data without considering outcomes. Mortality and microbiologic outcomes were then compared between subphenotypes.
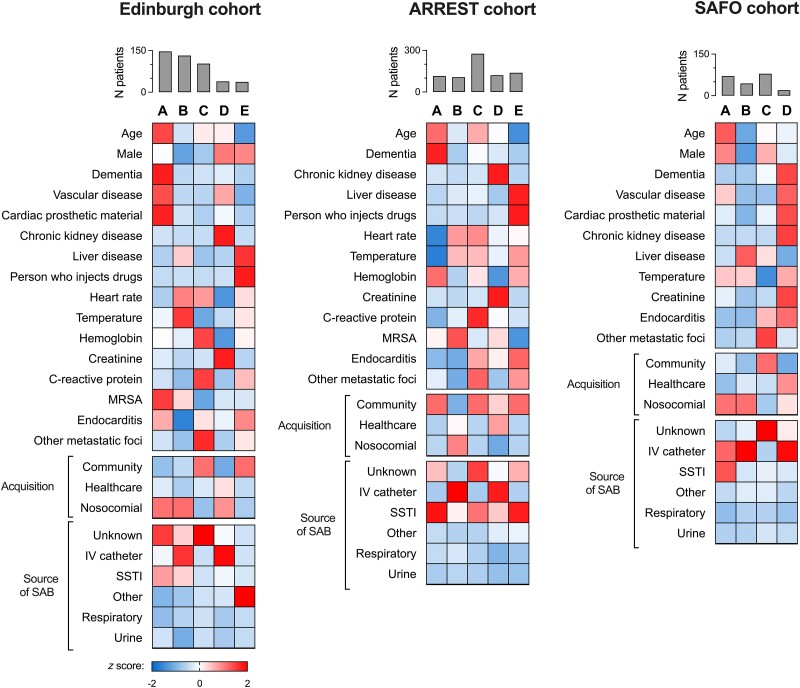
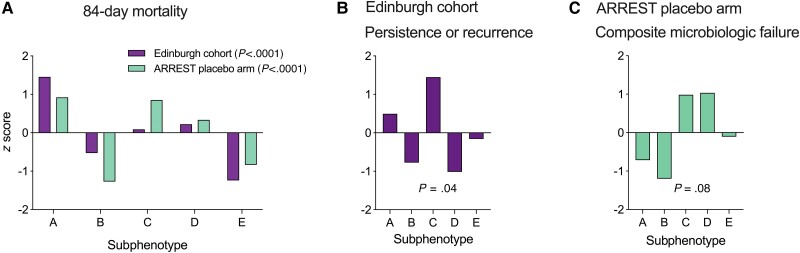
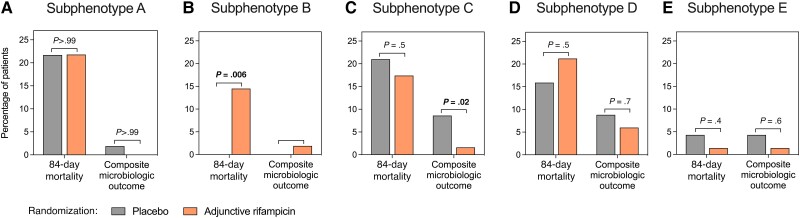
Results: Included patients had predominantly methicillin-susceptible SAB (1366 of 1430, 95.5%). We identified 5 distinct, reproducible clinical subphenotypes: (A) SAB associated with older age and comorbidity, (B) nosocomial intravenous catheter-associated SAB in younger people without comorbidity, (C) community-acquired metastatic SAB, (D) SAB associated with chronic kidney disease, and (E) SAB associated with injection drug use. Survival and microbiologic outcomes differed between the subphenotypes. Mortality was highest in subphenotype A and lowest in subphenotypes B and E. Microbiologic outcomes were worse in subphenotype C. In a secondary analysis of the ARREST trial, adjunctive rifampicin was associated with increased mortality in subphenotype B and improved microbiologic outcomes in subphenotype C.
Conclusions: We have identified reproducible and clinically relevant subphenotypes within SAB and provide proof of principle of differential treatment effects. Through clinical trial enrichment and patient stratification, these subphenotypes could contribute to a personalized medicine approach to SAB.
Keywords: Staphylococcus aureus; adjunctive treatment; bacteraemia; patient stratification; subphenotypes.
© The Author(s) 2024. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest . C. T. reports speaker fees from Gedeon Richter. V. G. F. reports grants/research support from Astra Zeneca, MedImmune, Merck, ContraFect, Karius, Genentech, Regeneron, and Basilea; serving as a paid consultant for Astra Zeneca, GSK, Armata, Debiopharm, Genentech, Basilea Affinergy, Janssen, ContraFect, and Destiny; and royalties from UpToDate. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- Wilson R, Hamburger M. Fifteen years' experience with staphylococcus septicemia in a large city hospital; analysis of fifty-five cases in the Cincinnati General Hospital 1940 to 1954. Am J Med 1957; 22:437–57. - PubMed
-
- Bai AD, Lo CKL, Komorowski AS, et al. Staphylococcus aureus bacteraemia mortality: a systematic review and meta-analysis. Clin Microbiol Infect 2022; 28:1076–84. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
