

The interplay between birth weight and obesity in determining childhood and adolescent cardiometabolic risk
- PMID: 38918147
- PMCID: PMC11293585
- DOI: 10.1016/j.ebiom.2024.105205
The interplay between birth weight and obesity in determining childhood and adolescent cardiometabolic risk
Abstract
Background: Birth weight (BW) is associated with risk of cardiometabolic disease (CMD) in adulthood, which may depend on the state of obesity, in particular if developed at a young age. We hypothesised that BW and a polygenic score (PGS) for BW were associated with cardiometabolic risk and related plasma protein levels in children and adolescents. We aimed to determine the modifying effect of childhood obesity on these associations.
Methods: We used data from The cross-sectional HOLBAEK Study with 4263 participants (median [IQR] age, 11.7 [9.2, 14.3] years; 57.1% girls and 42.9% boys; 48.6% from an obesity clinic and 51.4% from a population-based group). We gathered information on BW and gestational age, anthropometrics, cardiometabolic risk factors, calculated a PGS for BW, and measured plasma proteins using Olink Inflammation and Cardiovascular II panels. We employed multiple linear regression to examine the associations with BW as a continuous variable and performed interaction analyses to assess the effect of childhood obesity on cardiometabolic risk and plasma protein levels.
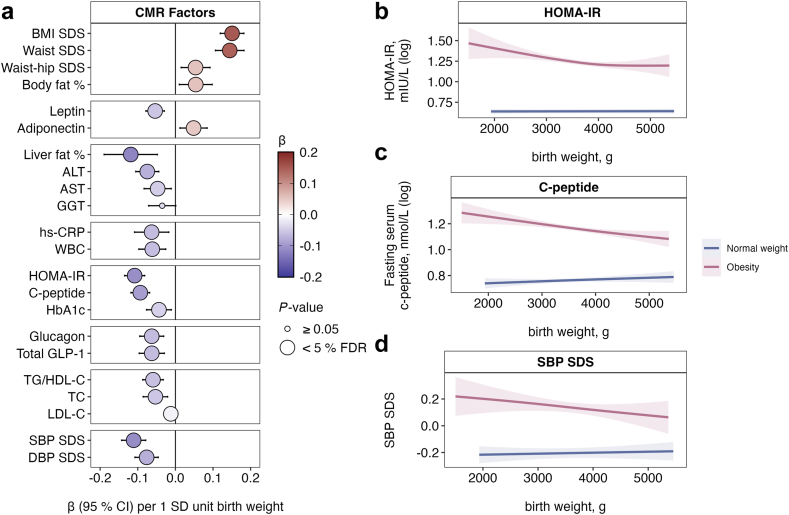
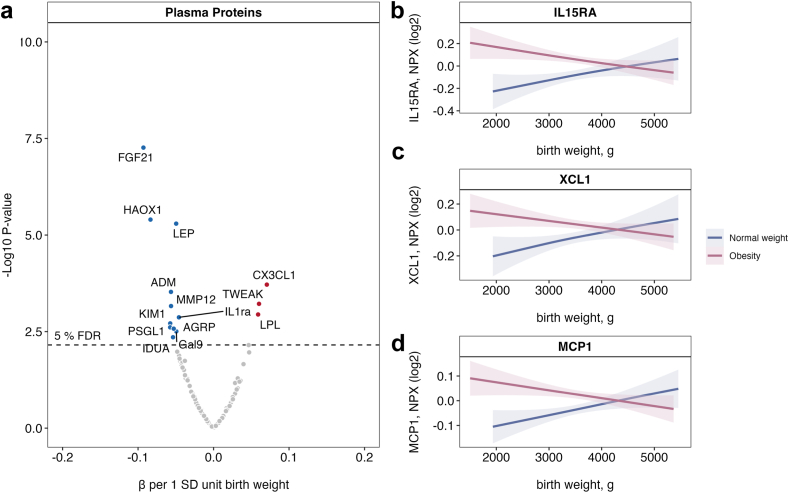
Findings: BW and a PGS for BW associated with cardiometabolic risk and plasma protein levels in childhood and adolescence. Childhood obesity modified the associations between BW and measures of insulin resistance, including HOMA-IR (βadj [95% CI per SD] for obesity: -0.12 [-0.15, -0.08]; normal weight: -0.04 [-0.08, 0.00]; Pinteraction = 0.004), c-peptide (obesity: -0.11 [-0.14, -0.08]; normal weight: -0.02 [-0.06, 0.02]; Pinteraction = 5.05E-04), and SBP SDS (obesity: -0.12 [-0.16, -0.08]; normal weight: -0.06 [-0.11, -0.01]; Pinteraction = 0.0479). Childhood obesity also modified the associations between BW and plasma levels of 14 proteins (e.g., IL15RA, MCP1, and XCL1; Pinteraction < 0.05).
Interpretation: We identified associations between lower BW and adverse metabolic phenotypes, particularly insulin resistance, blood pressure, and altered plasma protein levels, which were more pronounced in children with obesity. Developing effective prevention and treatment strategies for this group is needed to reduce the risk of future CMD.
Funding: Novo Nordisk Foundation (NNF15OC0016544, NNF0064142 to T.H., NNF15OC0016692 to T.H. and A.K., NNF18CC0033668 to S.E.S, NNF18SA0034956 to C.E.F., NNF20SA0067242 to DCA, NNF18CC0034900 to NNF CBMR), The Innovation Fund Denmark (0603-00484B to T.H.), The Danish Cardiovascular Academy (DCA) and the Danish Heart Foundation (HF) (PhD2021007-DCA to P.K.R, 18-R125-A8447-22088 (HF) and 21-R149-A10071-22193 (HF) to M.A.V.L., PhD2023009-HF to L.A.H), EU Horizon (668031, 847989, 825694, 964590 to A.K.), Innovative Health Initiative (101132901 for A.K.), A.P. Møller Foundation (19-L-0366 to T.H.), The Danish National Research Foundation, Steno Diabetes Center Sjælland, and The Region Zealand and Southern Denmark Health Scientific Research Foundation.
Keywords: Adolescent; Birth weight; Child; Inflammation; Obesity; Polygenic score.
Copyright © 2024 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests C.E.F. has received speaker honoria from The Danish Society for General Practice, Novo Nordisk, Nestlé and payment for manuscript writing from The Danish Health Authority. C.B. and T.H. have stocks in Novo Nordisk. A.K. receives royalties from Gyldendal, payment for lectures from Norgine, Siemens, Nordic Bioscience, Novo Nordisk. A.K. has two patents planned/pending, participates on an advisory board for Norgine, Siemens, Novo Nordisk, B&I. A.K. has a leadership role as the Secretary General European Association for the Study of The Liver (EASL) 2023–2025. A.K. has received equipment, materials, and drugs from Norgine (Rifaximin), Siemens (ELF Test), Echosence (FibroScan), and Nordic Bioscience (ECM markers). A.K. has finical interest as the Board member and co-founder Evido. J-C.H. has received payment for expert testimony from Novo Nordisk and support for meetings and travel from Rhytm, provides training and treatment of obesity. We declare no other competing interests from remaining coauthors.
Figures

References
-
- Mericq V., Martinez-Aguayo A., Uauy R., Iñiguez G., Van der Steen M., Hokken-Koelega A. Long-term metabolic risk among children born premature or small for gestational age. Nat Rev Endocrinol. 2017;13:50–62. - PubMed
-
- Zhao Y., Wang S.-F., Mu M., Sheng J. Birth weight and overweight/obesity in adults: a meta-analysis. Eur J Pediatr. 2012;171:1737–1746. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
