

Which factors are associated with adverse prognosis in multiple myeloma patients after surgery? - preliminary establishment and validation of the nomogram
- PMID: 38918829
- PMCID: PMC11202362
- DOI: 10.1186/s12957-024-03453-y
Which factors are associated with adverse prognosis in multiple myeloma patients after surgery? - preliminary establishment and validation of the nomogram
Abstract
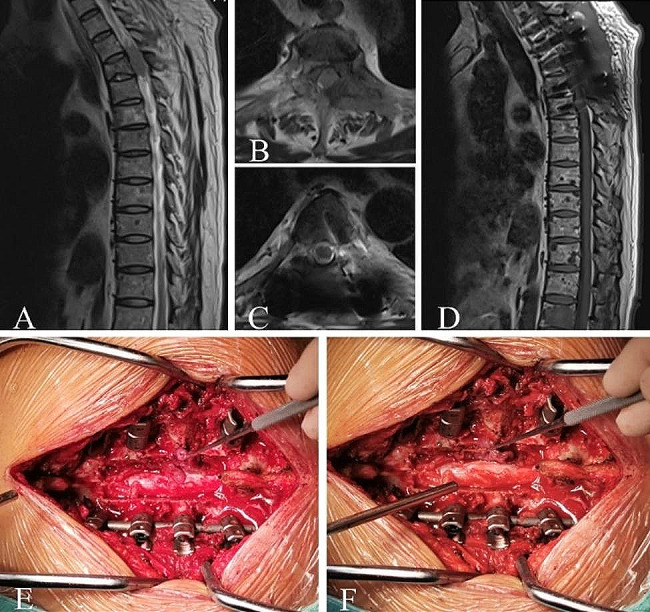
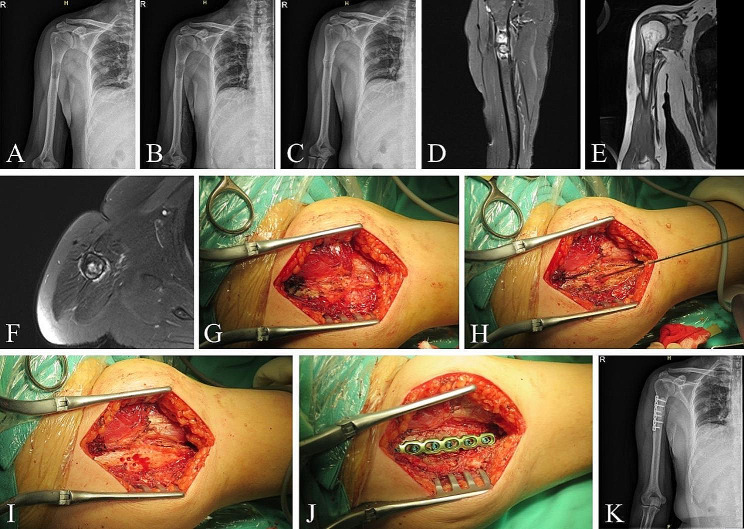
Background: To investigate the prognosis of patients with Multiple Myeloma (MM) after surgery, analyze the risk factors leading to adverse postoperative outcomes, and establish a nomogram.
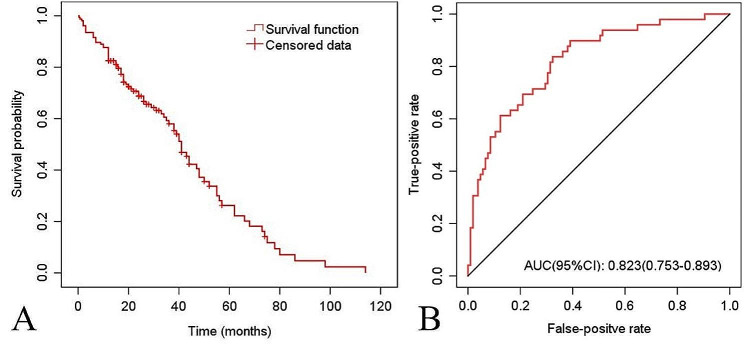
Methods: Clinical data from 154 patients with MM who underwent surgery at our institution between 2007 and 2019 were retrospectively analyzed. Assessing and comparing patients' pain levels, quality of life, and functional status before and after surgery (P < 0.05) were considered statistically significant. The Kaplan-Meier survival curve was used to estimate the median survival time. Adverse postoperative outcomes were defined as worsened symptoms, lesion recurrence, complication grade ≥ 2, or a postoperative survival period < 1 year. Logistic regression analysis was used to determine the prognostic factors. Based on the logistic regression results, a nomogram predictive model was developed and calibrated.
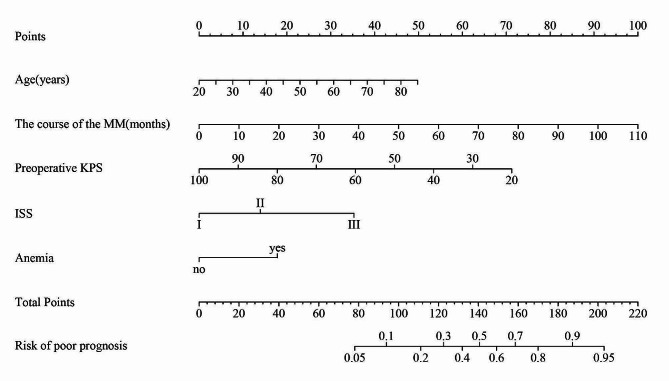
Results: Postoperative pain was significantly alleviated in patients with MM, and there were significant improvements in the quality of life and functional status (P < 0.05). The median postoperative survival was 41 months. Forty-nine patients (31.8%) experienced adverse postoperative outcomes. Multivariate logistic regression analysis identified patient age, duration of MM, International Staging System, preoperative Karnofsky Performance Status, and Hb < 90 g/L as independent factors influencing patient prognosis. Based on these results, a nomogram was constructed, with a C-index of 0.812. The calibration curve demonstrated similarity between the predicted and actual survival curves. Decision curve analysis favored the predictive value of the model at high-risk thresholds from 10% to-69%.
Conclusion: This study developed a nomogram risk prediction model to assist in providing quantifiable assessment indicators for preoperative evaluation of surgical risk.
Keywords: Multiple myeloma; Nomogram; Prognosis; Surgery; Survival analysis.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

Similar articles
-
[Risk factor analysis on body mass rebound after laparoscopic sleeve gastrectomy and establishment of a nomogram prediction model].Zhonghua Wei Chang Wai Ke Za Zhi. 2022 Oct 25;25(10):913-920. doi: 10.3760/cma.j.cn441530-20220418-00159. Zhonghua Wei Chang Wai Ke Za Zhi. 2022. PMID: 36245117 Chinese.
-
[Construction and evaluation of a nomogram for predicting the prognosis of patients with colorectal cancer with peritoneal carcinomatosis treated with cytoreductive surgery plus hyperthermic intraperitoneal chemotherapy].Zhonghua Wei Chang Wai Ke Za Zhi. 2023 May 25;26(5):434-441. doi: 10.3760/cma.j.cn441530-20230309-00071. Zhonghua Wei Chang Wai Ke Za Zhi. 2023. PMID: 37217351 Chinese.
-
[Risk factor analysis on anastomotic leakage after laparoscopic surgery in rectal cancer patient with neoadjuvant therapy and establishment of a nomogram prediction model].Zhonghua Wei Chang Wai Ke Za Zhi. 2019 Aug 25;22(8):748-754. doi: 10.3760/cma.j.issn.1671-0274.2019.08.009. Zhonghua Wei Chang Wai Ke Za Zhi. 2019. PMID: 31422613 Chinese.
-
Pleural effusion-based nomogram to predict outcomes in unselected patients with multiple myeloma: a large single center experience.Ann Hematol. 2021 Jul;100(7):1789-1801. doi: 10.1007/s00277-021-04484-1. Epub 2021 Mar 14. Ann Hematol. 2021. PMID: 33715037
-
Prognostic nomogram incorporating cytokines for overall survival in patients with newly diagnosed multiple myeloma.Int Immunopharmacol. 2021 Oct;99:108016. doi: 10.1016/j.intimp.2021.108016. Epub 2021 Aug 9. Int Immunopharmacol. 2021. PMID: 34385029
References
-
- Terpos E, Zamagni E, Lentzsch S, Drake MT, García-Sanz R, Abildgaard N, Ntanasis-Stathopoulos I, Schjesvold F, Rubia Jdl, Kyriakou C, et al. Treatment of multiple myeloma-related bone disease: recommendations from the Bone Working Group of the International Myeloma Working Group. Lancet Oncol. 2021;22:e119–30. doi: 10.1016/S1470-2045(20)30559-3. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
