

S100 proteins as potential predictive biomarkers of abatacept response in polyarticular juvenile idiopathic arthritis
- PMID: 38918871
- PMCID: PMC11197242
- DOI: 10.1186/s13075-024-03347-0
S100 proteins as potential predictive biomarkers of abatacept response in polyarticular juvenile idiopathic arthritis
Erratum in
-
Correction: S100 proteins as potential predictive biomarkers of abatacept response in polyarticular juvenile idiopathic arthritis.Arthritis Res Ther. 2024 Aug 31;26(1):154. doi: 10.1186/s13075-024-03385-8. Arthritis Res Ther. 2024. PMID: 39217348 Free PMC article. No abstract available.
Abstract
Background: Juvenile idiopathic arthritis (JIA) comprises a heterogeneous group of conditions that can cause marked disability and diminished quality of life. Data on predictors of clinical response are insufficient to guide selection of the appropriate biologic agent for individual patients. This study aimed to investigate the propensity of S100A8/9 and S100A12 as predictive biomarkers of abatacept response in polyarticular-course juvenile idiopathic arthritis (pJIA).
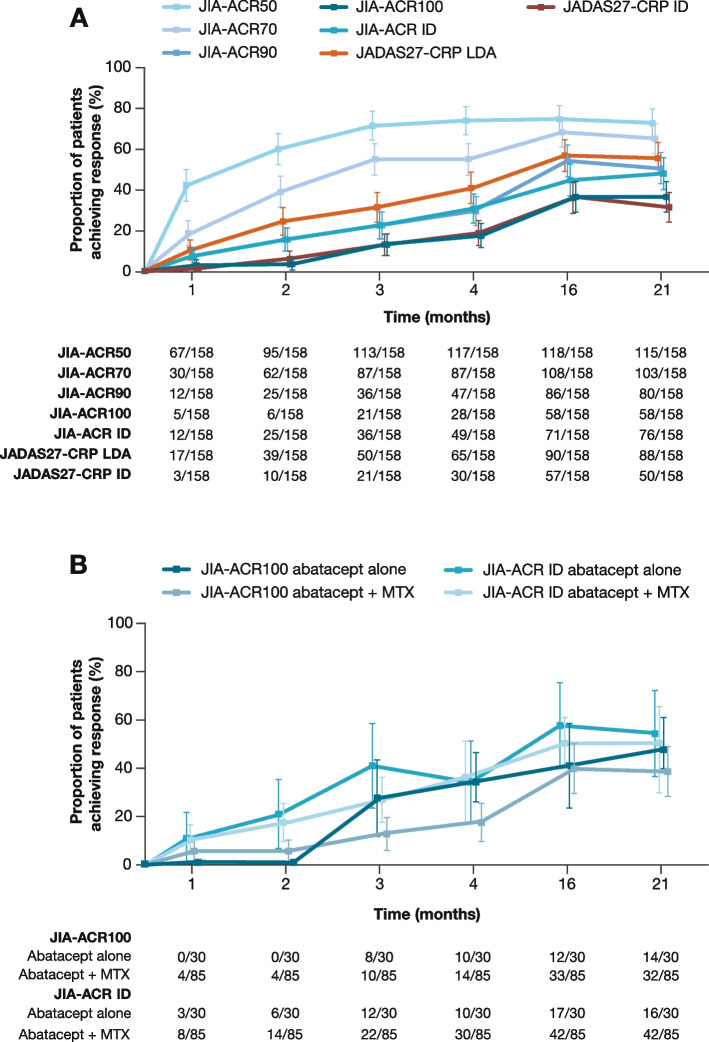
Methods: Data from a phase 3 trial (NCT01844518) of subcutaneous abatacept in patients with active pJIA (n = 219) were used in this exploratory analysis. Association between biomarker levels at baseline and improvements in JIA-American College of Rheumatology (ACR) criteria responses or baseline disease activity (measured by Juvenile Arthritis Disease Activity Score in 27 joints using C-reactive protein [JADAS27-CRP]) were assessed. Biomarker level changes from baseline to month 4 were assessed for disease outcome prediction up to 21 months.
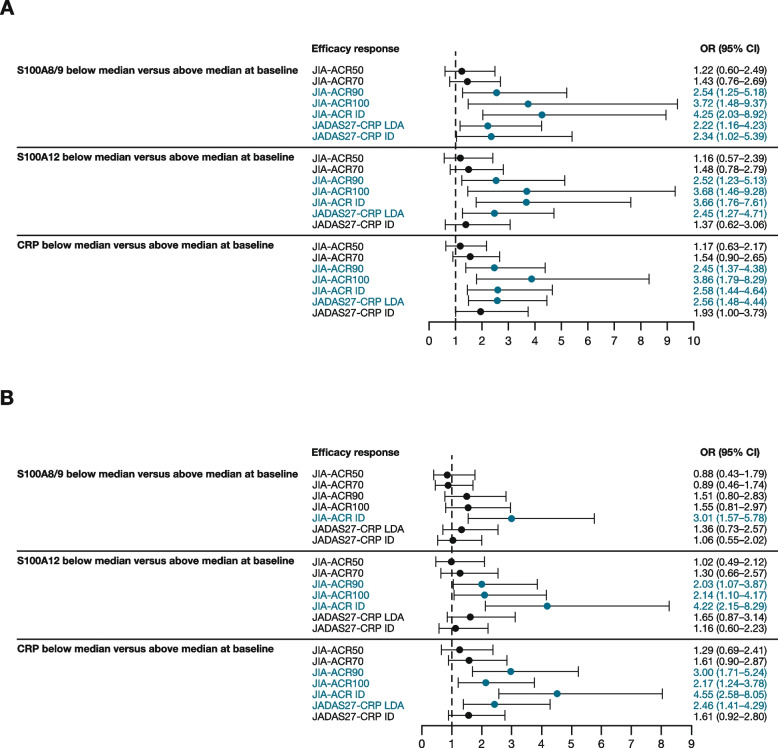
Results: At baseline, 158 patients had available biomarker samples. Lower baseline S100A8/9 levels (≤ 3295 ng/mL) were associated with greater odds of achieving JIA-ACR90 (odds ratio [OR]: 2.54 [95% confidence interval (CI): 1.25-5.18]), JIA-ACR100 (OR: 3.72 [95% CI: 1.48-9.37]), JIA-ACR inactive disease (ID; OR: 4.25 [95% CI: 2.03-8.92]), JADAS27-CRP ID (OR: 2.34 [95% CI: 1.02-5.39]) at month 4, and JIA-ACR ID (OR: 3.01 [95% CI: 1.57-5.78]) at month 16. Lower baseline S100A12 levels (≤ 176 ng/mL) were associated with greater odds of achieving JIA-ACR90 (OR: 2.52 [95% CI: 1.23-5.13]), JIA-ACR100 (OR: 3.68 [95% CI: 1.46-9.28]), JIA-ACR ID (OR: 3.66 [95% CI: 1.76-7.61]), JIA-ACR90 (OR: 2.03 [95% CI: 1.07-3.87]), JIA-ACR100 (OR: 2.14 [95% CI: 1.10-4.17]), and JIA-ACR ID (OR: 4.22 [95% CI: 2.15-8.29]) at month 16. From baseline to month 4, decreases in S100A8/9 and S100A12 generally exceeded 50% among JIA-ACR90/100/ID responders.
Conclusion: Lower baseline levels of S100A8/9 and S100A12 proteins predicted better response to abatacept treatment than higher levels and may serve as early predictive biomarkers in pJIA. Decreases in these biomarker levels may also predict longer-term response to abatacept in pJIA.
Keywords: Abatacept; Biomarkers; C-Reactive protein (CRP); Juvenile idiopathic arthritis; S100.
© 2024. The Author(s).
Conflict of interest statement
HIB: consultant: AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, GlaxoSmithKline, Janssen, Merck, Novartis, Pfizer, Roche, UCB (funds go to CCHMC/employer); grant/research support: Bristol Myers Squibb, Pfizer (funds go to CCHMC/employer). GSS: speakers bureau: Novartis; consultant: Sobi. GVC: speakers bureau: AbbVie; grant/research support: Bristol Myers Squibb, Eli Lilly, Janssen, Parexel, Sanofi. JA: speakers bureau: AbbVie, Gebro, GlaxoSmithKline, Novartis, Pfizer, Roche, Sobi; consultant: AbbVie, Gebro, GlaxoSmithKline, Novartis, Pfizer, Roche, Sobi; grant/research support: AbbVie, Amgen, Gebro, GlaxoSmithKline, Lilly, Novartis, Novimmune, Pfizer, Roche, Sanofi, Sobi. RC: speakers bureau: AbbVie, Bristol Myers Squibb, GlaxoSmithKline, Lilly, Novartis, Pfizer, Roche, UCB; paid instructor: AbbVie, Novartis, Pfizer, Roche; consultant: AbbVie, Bristol Myers Squibb, GlaxoSmithKline, Lilly, Novartis, Pfizer, Roche, UCB. IF: consultant: Bristol Myers Squibb, Gilead, Hexal, MEDAC, Novartis, Pfizer, Sanofi. DJK: consultant: Pfizer. MA: consultant: Bristol Myers Squibb (working for Syneos Health). JL: employee, shareholder: Bristol Myers Squibb. SM: shareholder: Bristol Myers Squibb; employee, shareholder: GlaxoSmithKline. RLW: employee (at the time of analysis): Bristol Myers Squibb; shareholder: Bristol Myers Squibb. DJL: speakers bureau: Genentech, Wyeth Pharm; consultant: Abbott, AstraZeneca, Boehringer Ingelheim, Celgene, F Hoffmann-La Roche, GlaxoSmithKline, Novartis, Pfizer, Regeneron, UBC, Wyeth Pharma. AM: speakers bureau: AbbVie, Novartis; consultant: AbbVie, Eli Lilly, EMD Serono, Idorsia, Janssen, Novartis, Pfizer. NR: honoraria, speakers bureau, consultant: Ablynx, AstraZeneca-Medimmune, Bayer, Biogen, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Eli Lilly, EMD Serono, F Hoffmann-La Roche, GlaxoSmithKline, Janssen, Merck, Novartis, Pfizer, R-Pharma, Sinergie, Sobi, UCB; grant/research support: The IRCCS Istituto Giannina Gaslini, where NR works as full-time public employee, has received contributions from: Bristol Myers Squibb, Eli Lilly, F Hoffmann-La Roche, GlaxoSmithKline, Janssen, Novartis, Pfizer, Sobi. This funding has been reinvested for the research activities of the hospital in a fully independent manner, without any commitment to third parties. AAG: consultant, grant/research support: AB2Bio, Novartis, Sobi (NovImmune). AS, ST, MH: none declared.
Figures

References
-
- Oliveira S, Ravelli A, Pistorio A, Castell E, Malattia C, Prieur AM, Saad Magalhães C, Murray KJ, Bae SC, Joos R, et al. Proxy-reported health-related quality of life of patients with juvenile idiopathic arthritis: the Pediatric Rheumatology International Trials Organization multinational quality of life cohort study. Arthritis Rheum. 2007;57(1):35–43. 10.1002/art.22473 - DOI - PubMed
-
- Ravelli A, Consolaro A, Horneff G, Laxer RM, Lovell DJ, Wulffraat NM, Akikusa JD, Al-Mayouf SM, Anton J, Avcin T, et al. Treating juvenile idiopathic arthritis to target: recommendations of an international task force. Ann Rheum Dis. 2018;77(6):819–28. - PubMed
-
- Ringold S, Angeles-Han ST, Beukelman T, Lovell D, Cuello CA, Becker ML, Colbert RA, Feldman BM, Ferguson PJ, Gewanter H. 2019 American College of Rheumatology/Arthritis Foundation guideline for the treatment of juvenile idiopathic arthritis: therapeutic approaches for non‐systemic polyarthritis, sacroiliitis, and enthesitis. Arthritis Care Res (Hoboken). 2019;71(6):717–34. 10.1002/acr.23870 - DOI - PMC - PubMed
-
- Ruperto N, Lovell DJ, Quartier P, Paz E, Rubio-Perez N, Silva CA, bud-Mendoza C, Burgos-Vargas R, Gerloni V, Melo-Gomes JA, et al. Abatacept in children with juvenile idiopathic arthritis: a randomised, double-blind, placebo-controlled withdrawal trial. Lancet. 2008;372(9636):383–91. 10.1016/S0140-6736(08)60998-8 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
