

Radiation Oncologists' Perspectives on Oligometastatic Prostate Cancer: A Survey from Korean Oligometastasis Working Group
- PMID: 38920729
- PMCID: PMC11203304
- DOI: 10.3390/curroncol31060245
Radiation Oncologists' Perspectives on Oligometastatic Prostate Cancer: A Survey from Korean Oligometastasis Working Group
Abstract
Background: Interest in the oligometastatic prostate cancer (OMPC) is increasing, and various clinical studies have reported the benefits of metastasis-directed radiation therapy (MDRT) in OMPC. However, the recognition regarding the adopted definitions, methodologies of assessment, and therapeutic approaches is diverse among radiation oncologists. This study aims to evaluate the level of agreement for issues in OMPC among radiation oncologists.
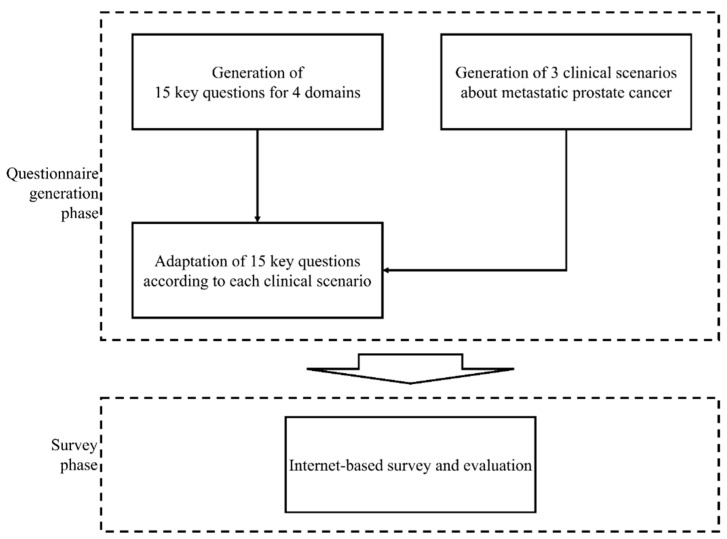
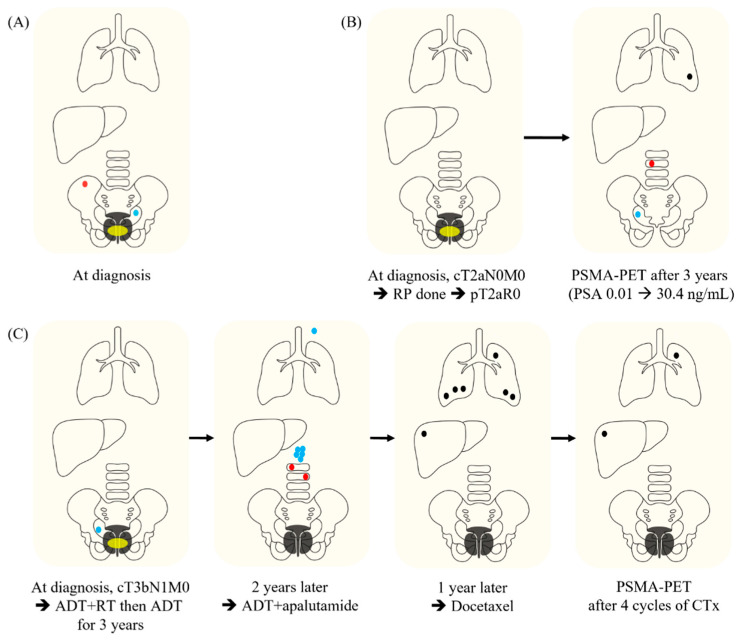
Methods: We generated 15 key questions (KQs) for OMPC relevant to definition, diagnosis, local therapies, and endpoints. Additionally, three clinical scenarios representing synchronous metastatic prostate cancer (mPC) (case 1), metachronous mPC with visceral metastasis (case 2), and metachronous mPC with castration-resistance and history of polymetastasis (case 3) were developed. The 15 KQs were adapted according to each scenario and transformed into 23 questions with 6-9 per scenario. The survey was distributed to 80 radiation oncologists throughout the Republic of Korea. Answer options with 0.0-29.9%, 30-49.9%, 50-69.9%, 70-79.9%, 80-89.9%, and 90-100% agreements were considered as no, minimal, weak, moderate, strong, and near perfect agreement, respectively.
Results: Forty-five candidates voluntarily participated in this study. Among 23 questions, near perfect (n = 4), strong (n = 3), or moderate (n = 2) agreements were shown in nine. For the case recognized as OMPC with agreements of 93% (case 1), near perfect agreements on the application of definitive radiation therapy (RT) for whole metastatic lesions were achieved. While ≥70% agreements regarding optimal dose-fractionation for metastasis-directed RT (MDRT) has not been achieved, stereotactic body RT (SBRT) is favored by clinicians with higher clinical volume.
Conclusion: For the case recognized as OMPC, near perfect agreement for the application of definitive RT for whole metastatic lesions was reached. SBRT was more favored as a MDRT by clinicians with a higher clinical volume.
Keywords: local therapy; oligometastasis; prostate cancer; radiation therapy; survey study.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Radiotherapy in oligometastatic prostate cancer-a pattern of care survey among members of the German Society for Radiation Oncology (DEGRO).Strahlenther Onkol. 2022 Aug;198(8):727-734. doi: 10.1007/s00066-022-01925-2. Epub 2022 Apr 1. Strahlenther Onkol. 2022. PMID: 35364690 Free PMC article.
-
Radiation Oncologists' Perspectives on Oligometastatic Disease: A Korean Survey Study.Cancer Res Treat. 2024 Apr;56(2):414-421. doi: 10.4143/crt.2023.876. Epub 2023 Nov 22. Cancer Res Treat. 2024. PMID: 37997326 Free PMC article.
-
Protocol for Evaluating the Efficacy and Safety of Radiotherapy for Prostate and Oligometastatic Lesions in Patients With Low-Burden Sensitive Oligometastatic Prostate Cancer: An Open, Exploratory Pilot Clinical Trial.Cancer Control. 2024 Jan-Dec;31:10732748241274595. doi: 10.1177/10732748241274595. Cancer Control. 2024. PMID: 39180187 Free PMC article.
-
Current Treatment Paradigms and Clinical Outcomes in Oligometastatic Prostate Cancer Patients: A Targeted Literature Review.Eur Urol Oncol. 2024 Dec;7(6):1280-1292. doi: 10.1016/j.euo.2024.06.002. Epub 2024 Jul 3. Eur Urol Oncol. 2024. PMID: 38964996 Review.
-
Oligometastatic Prostate Cancer: Results of a Dutch Multidisciplinary Consensus Meeting.Eur Urol Oncol. 2020 Apr;3(2):231-238. doi: 10.1016/j.euo.2019.07.010. Epub 2019 Aug 8. Eur Urol Oncol. 2020. PMID: 31401014
Cited by
-
Treatment Strategies in Oligo-Metastatic Prostate Cancer: A Nationwide Survey.Urol Int. 2025 Apr 14:1-10. doi: 10.1159/000545630. Online ahead of print. Urol Int. 2025. PMID: 40228489 Free PMC article.
References
-
- Lievens Y., Guckenberger M., Gomez D., Hoyer M., Iyengar P., Kindts I., Mendez Romero A., Nevens D., Palma D., Park C., et al. Defining oligometastatic disease from a radiation oncology perspective: An ESTRO-ASTRO consensus document. Radiother. Oncol. 2020;148:157–166. doi: 10.1016/j.radonc.2020.04.003. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
