

Multivitamin Use and Mortality Risk in 3 Prospective US Cohorts
- PMID: 38922615
- PMCID: PMC11208972
- DOI: 10.1001/jamanetworkopen.2024.18729
Multivitamin Use and Mortality Risk in 3 Prospective US Cohorts
Abstract
Importance: One in 3 US adults uses multivitamins (MV), with a primary motivation being disease prevention. In 2022, the US Preventive Services Task Force reviewed data on MV supplementation and mortality from randomized clinical trials and found insufficient evidence for determining benefits or harms owing, in part, to limited follow-up time and external validity.
Objective: To estimate the association of MV use with mortality risk, accounting for confounding by healthy lifestyle and reverse causation whereby individuals in poor health initiate MV use.
Design, setting, and participants: This cohort study used data from 3 prospective cohort studies in the US, each with baseline MV use (assessed from 1993 to 2001), and follow-up MV use (assessed from 1998 to 2004), extended duration of follow-up up to 27 years, and extensive characterization of potential confounders. Participants were adults, without a history of cancer or other chronic diseases, who participated in National Institutes of Health-AARP Diet and Health Study (327 732 participants); Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial (42 732 participants); or Agricultural Health Study (19 660 participants). Data were analyzed from June 2022 to April 2024.
Exposure: Self-reported MV use.
Main outcomes and measures: The main outcome was mortality. Cox proportional hazard models were used to estimate hazard ratios (HRs) and 95% CIs.
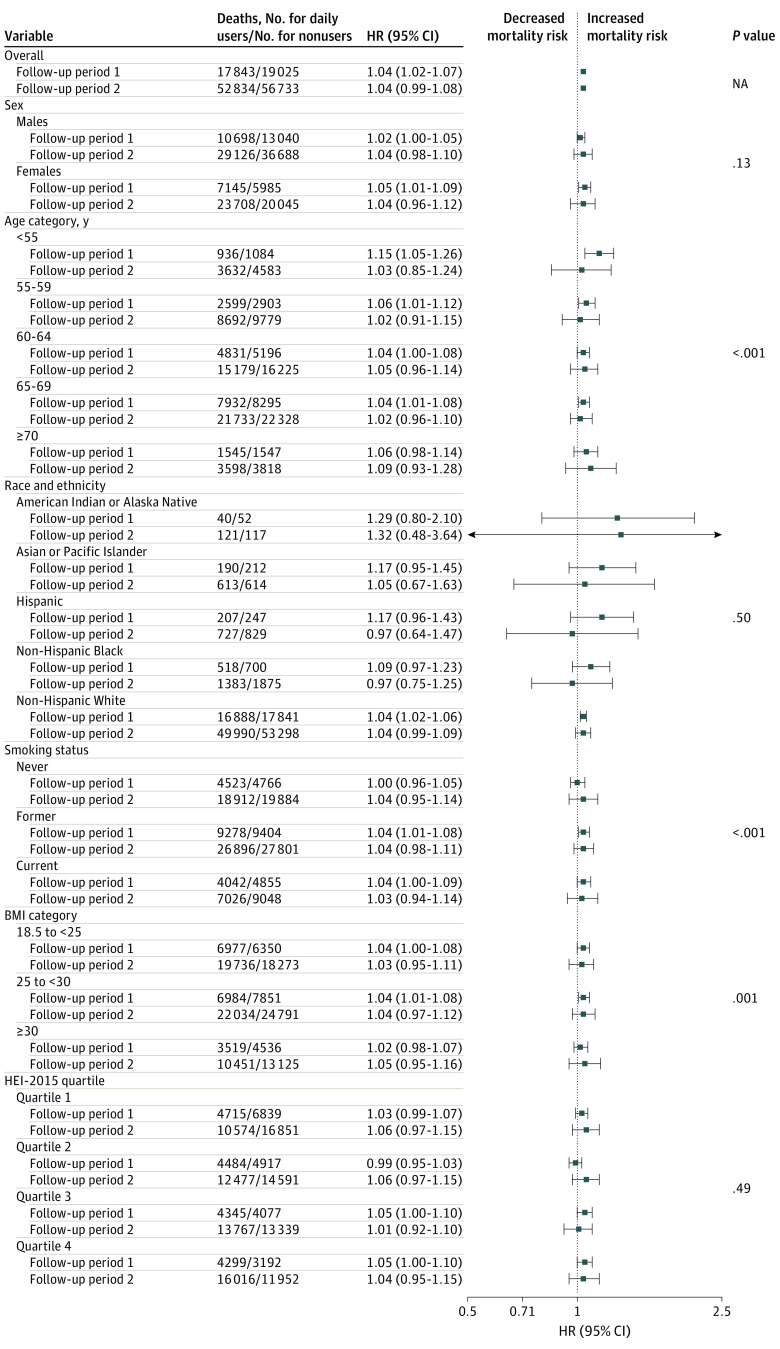
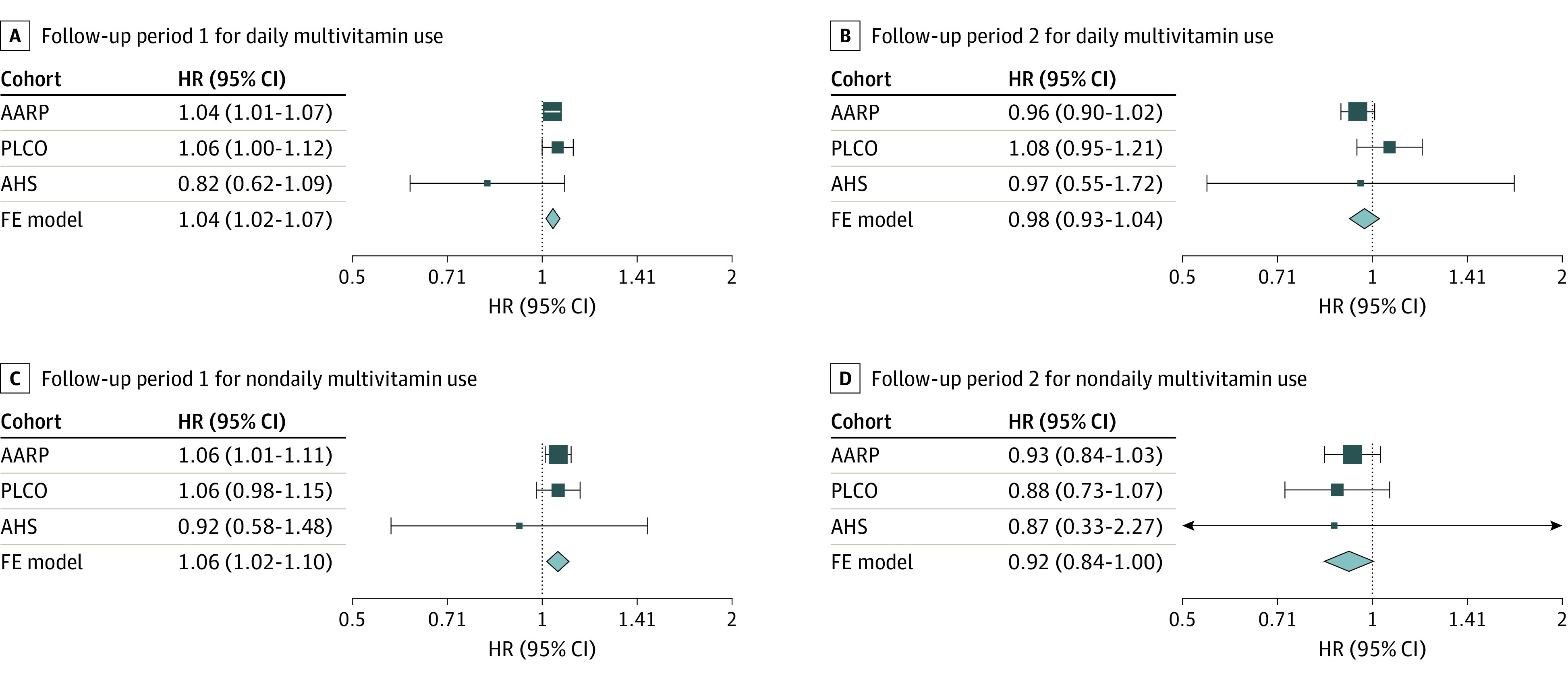
Results: Among 390 124 participants (median [IQR] age, 61.5 [56.7-66.0] years; 216 202 [55.4%] male), 164 762 deaths occurred during follow-up; 159 692 participants (40.9%) were never smokers, and 157 319 participants (40.3%) were college educated. Among daily MV users, 49.3% and 42.0% were female and college educated, compared with 39.3% and 37.9% among nonusers, respectively. In contrast, 11.0% of daily users, compared with 13.0% of nonusers, were current smokers. MV use was not associated with lower all-cause mortality risk in the first (multivariable-adjusted HR, 1.04; 95% CI, 1.02-1.07) or second (multivariable-adjusted HR, 1.04; 95% CI, 0.99-1.08) halves of follow-up. HRs were similar for major causes of death and time-varying analyses.
Conclusions and relevance: In this cohort study of US adults, MV use was not associated with a mortality benefit. Still, many US adults report using MV to maintain or improve health.
Conflict of interest statement
Figures
Comment in
-
The Limited Value of Multivitamin Supplements.JAMA Netw Open. 2024 Jun 3;7(6):e2418965. doi: 10.1001/jamanetworkopen.2024.18965. JAMA Netw Open. 2024. PMID: 38922621 No abstract available.
References
-
- Mangione CM, Barry MJ, Nicholson WK, et al. ; US Preventive Services Task Force . Vitamin, mineral, and multivitamin supplementation to prevent cardiovascular disease and cancer: US Preventive Services Task Force recommendation statement. JAMA. 2022;327(23):2326-2333. doi:10.1001/jama.2022.8970 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
