

Population-Based Risk of Psychiatric Disorders Associated With Recurrent Copy Number Variants
- PMID: 38922630
- PMCID: PMC11209205
- DOI: 10.1001/jamapsychiatry.2024.1453
Population-Based Risk of Psychiatric Disorders Associated With Recurrent Copy Number Variants
Abstract
Importance: Recurrent copy number variants (rCNVs) have been associated with increased risk of psychiatric disorders in case-control studies, but their population-level impact is unknown.
Objective: To provide unbiased population-based estimates of prevalence and risk associated with psychiatric disorders for rCNVs and to compare risks across outcomes, rCNV dosage type (deletions or duplications), and locus features.
Design, setting, and participants: This genetic association study is an analysis of data from the Lundbeck Foundation Initiative for Integrative Psychiatric Research (iPSYCH) case-cohort sample of individuals born in Denmark in 1981-2008 and followed up until 2015, including (1) all individuals (n = 92 531) with a hospital discharge diagnosis of attention-deficit/hyperactivity disorder (ADHD), autism spectrum disorder (ASD), bipolar disorder, major depressive disorder (MDD), or schizophrenia spectrum disorder (SSD) and (2) a subcohort (n = 50 625) randomly drawn from the source population. Data were analyzed from January 2021 to August 2023.
Exposures: Carrier status of deletions and duplications at 27 autosomal rCNV loci was determined from neonatal blood samples genotyped on single-nucleotide variant microarrays.
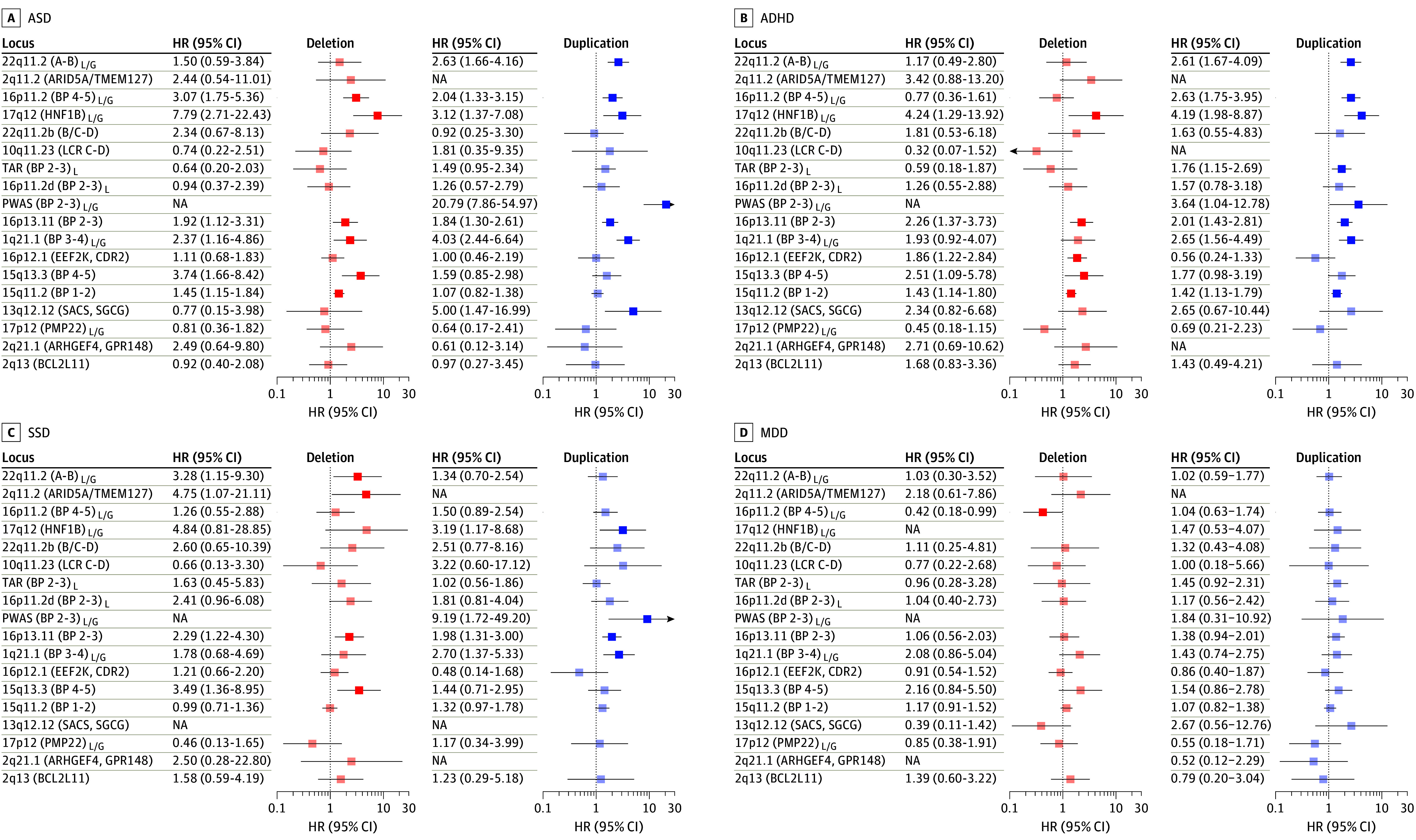
Main outcomes and measures: Population-based rCNV prevalence was estimated with a survey model using finite population correction to account for oversampling of cases. Hazard ratio (HR) estimates and 95% CIs for psychiatric disorders were derived using weighted Cox proportional hazard models. Risks were compared across outcomes, dosage type, and locus features using generalized estimating equation models.
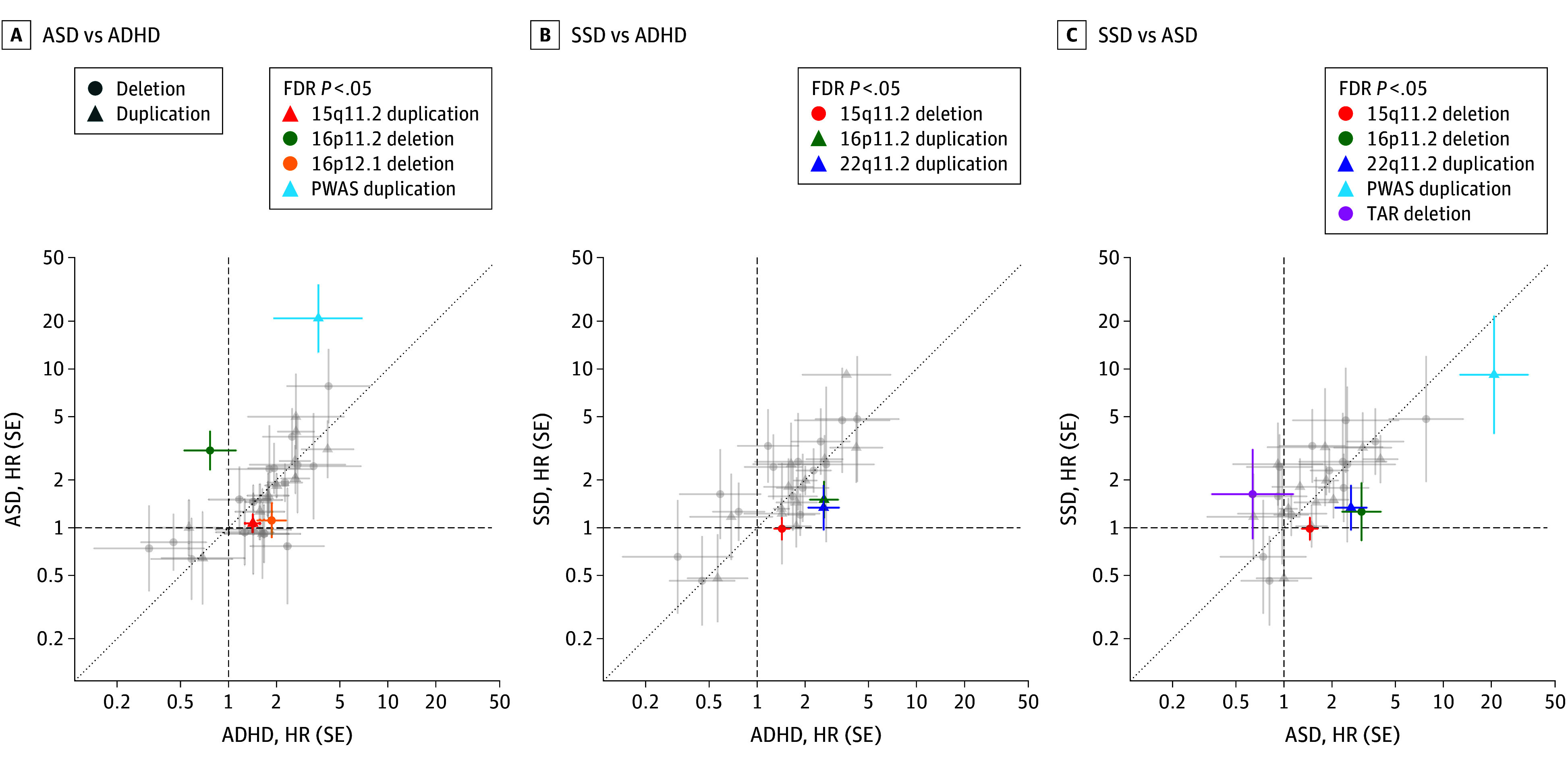
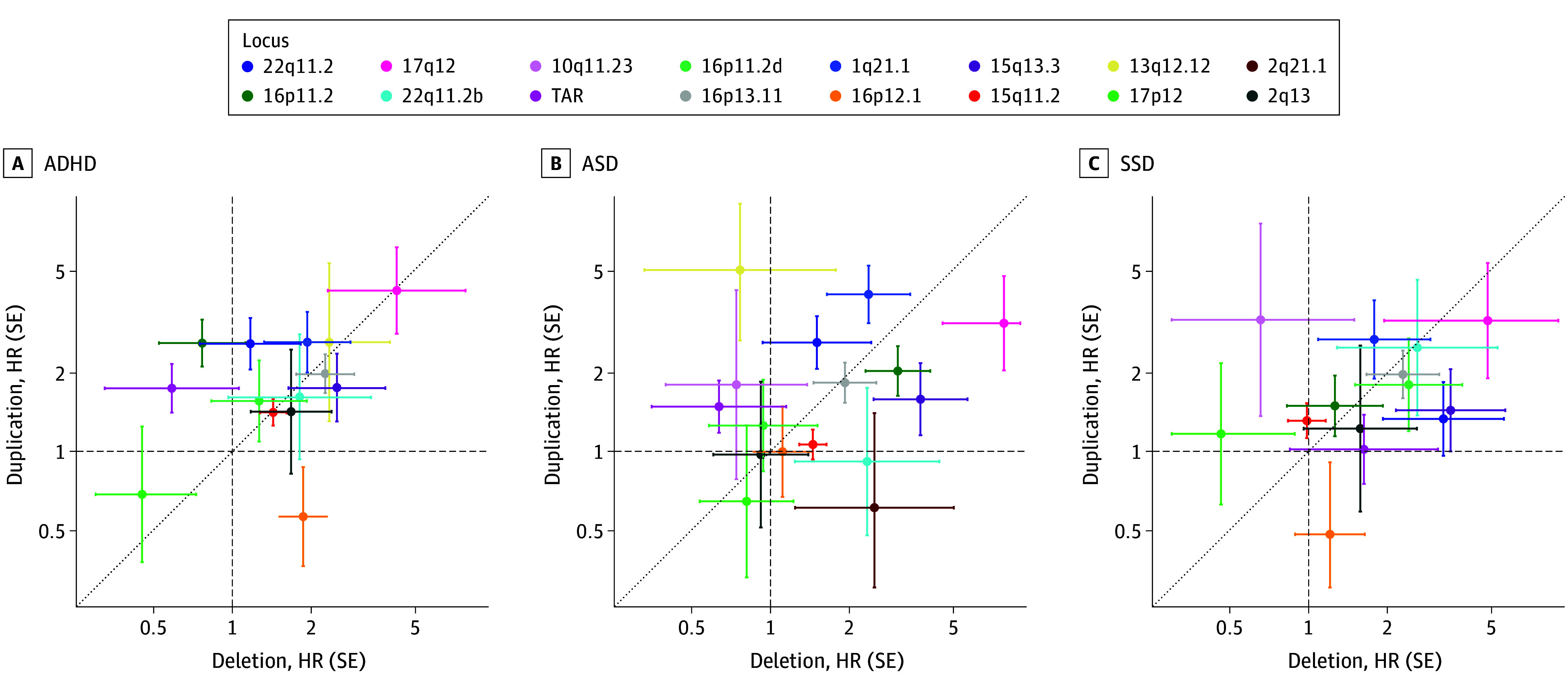
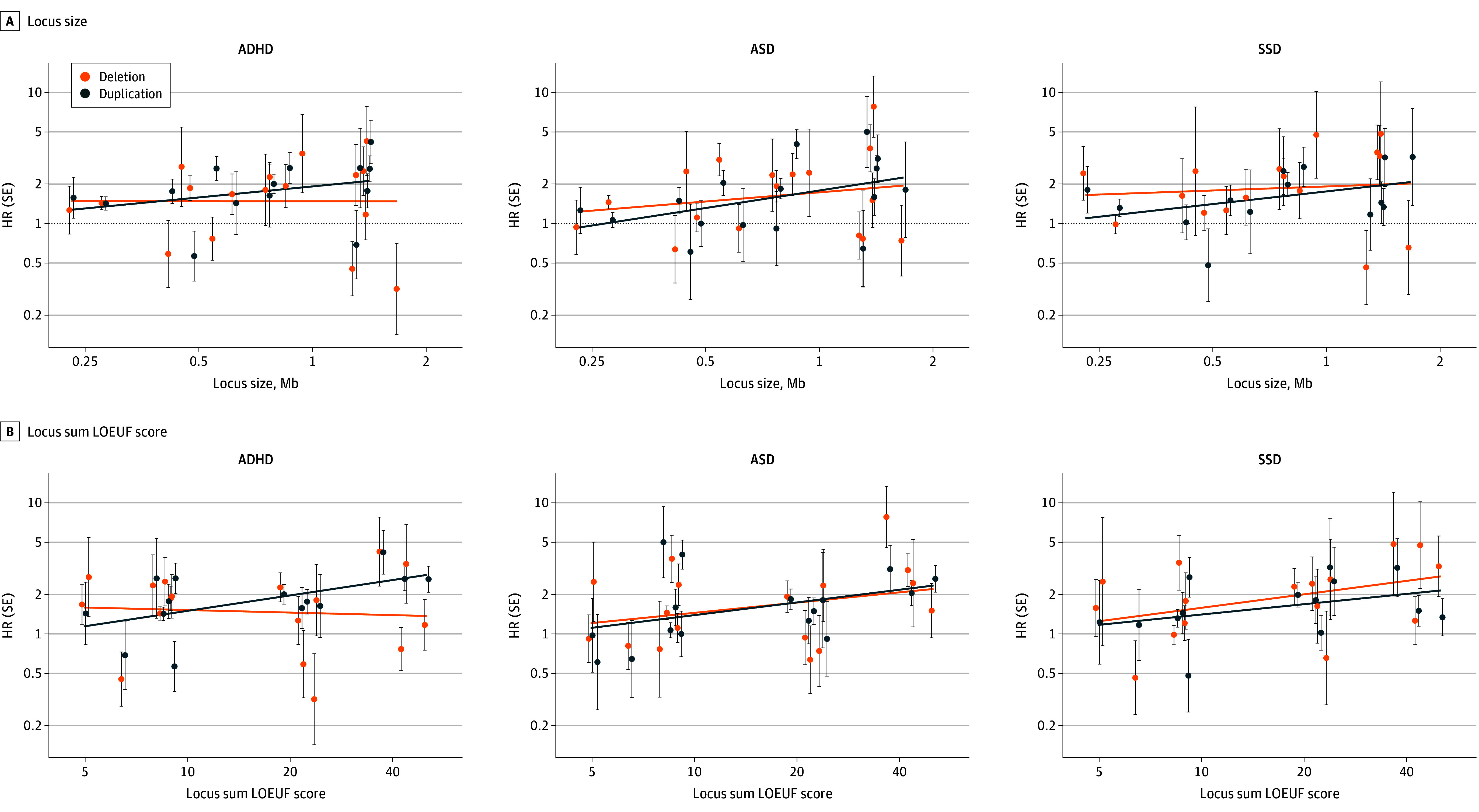
Results: A total of 3547 rCNVs were identified in 64 735 individuals assigned male at birth (53.8%) and 55 512 individuals assigned female at birth (46.2%) whose age at the end of follow-up ranged from 7.0 to 34.7 years (mean, 21.8 years). Most observed increases in rCNV-associated risk for ADHD, ASD, or SSD were moderate, and risk estimates were highly correlated across these disorders. Notable exceptions included high ASD-associated risk observed for Prader-Willi/Angelman syndrome duplications (HR, 20.8; 95% CI, 7.9-55). No rCNV was associated with increased MDD risk. Also, rCNV-associated risk was positively correlated with locus size and gene constraint but not with dosage type. Comparison with published case-control and community-based studies revealed a higher prevalence of deletions and lower associated increase in risk for several rCNVs in iPSYCH2015.
Conclusions and relevance: This study found that several rCNVs were more prevalent and conferred less risk of psychiatric disorders than estimated previously. Most case-control studies overestimate rCNV-associated risk of psychiatric disorders, likely because of selection bias. In an era where genetics is increasingly being clinically applied, these results highlight the importance of population-based risk estimates for genetics-based predictions.
Conflict of interest statement
Figures

Update of
-
Population-based Risk of Psychiatric Disorders Associated with Recurrent CNVs.medRxiv [Preprint]. 2023 Sep 5:2023.09.04.23294975. doi: 10.1101/2023.09.04.23294975. medRxiv. 2023. Update in: JAMA Psychiatry. 2024 Oct 1;81(10):957-966. doi: 10.1001/jamapsychiatry.2024.1453. PMID: 37886536 Free PMC article. Updated. Preprint.
