

Transcobalamin receptor antibodies in autoimmune vitamin B12 central deficiency
- PMID: 38924428
- PMCID: PMC11520464
- DOI: 10.1126/scitranslmed.adl3758
Transcobalamin receptor antibodies in autoimmune vitamin B12 central deficiency
Abstract
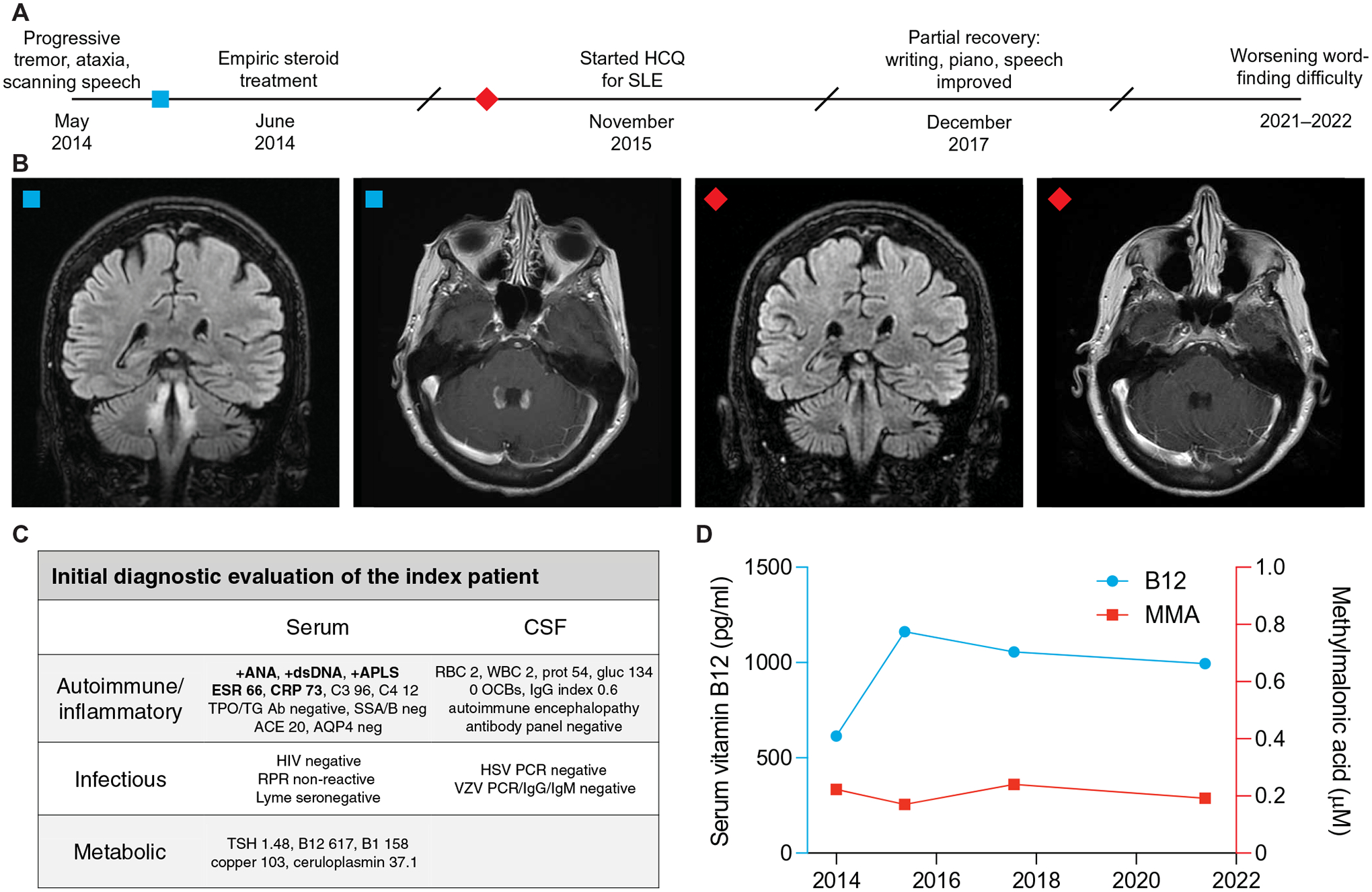
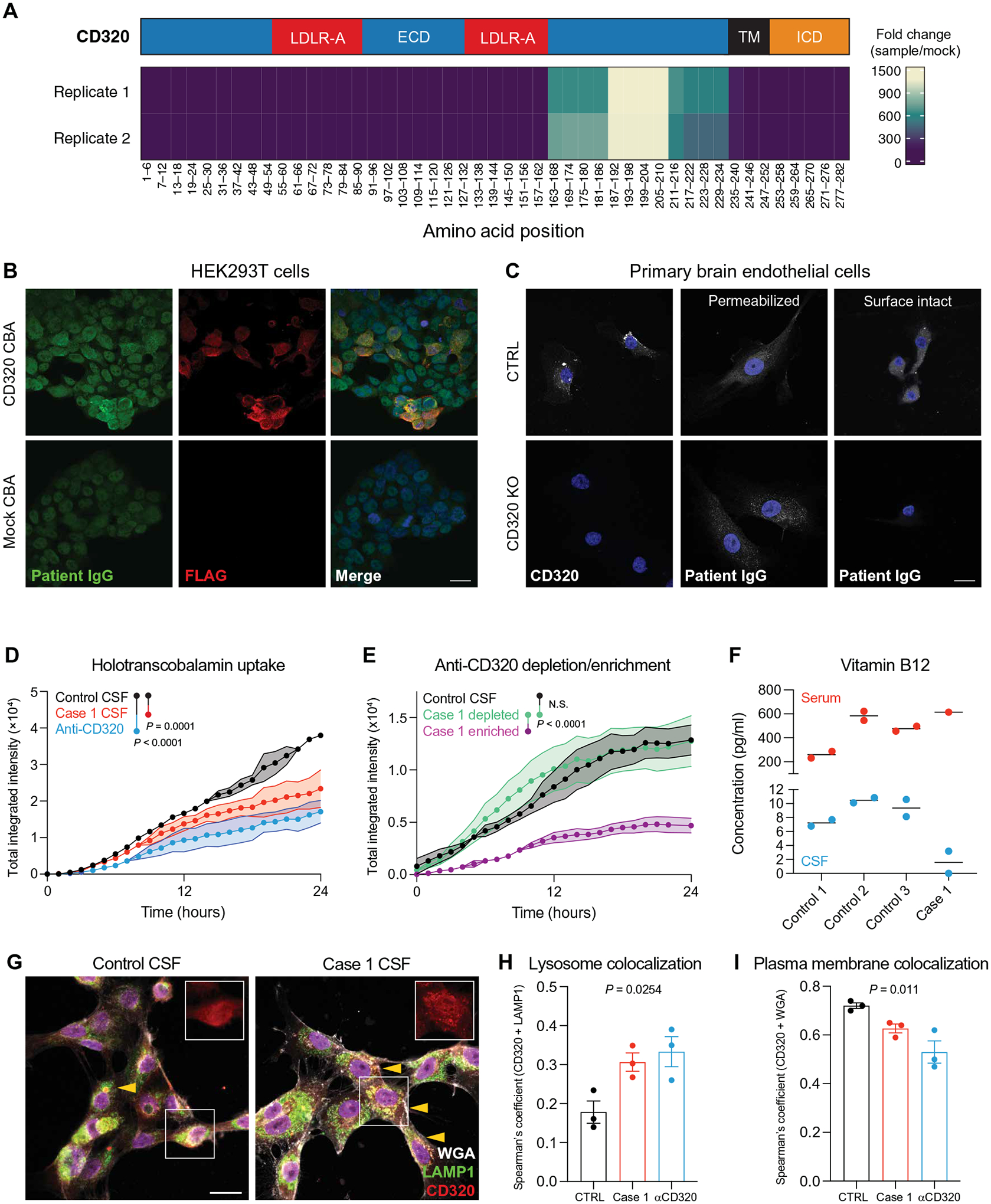
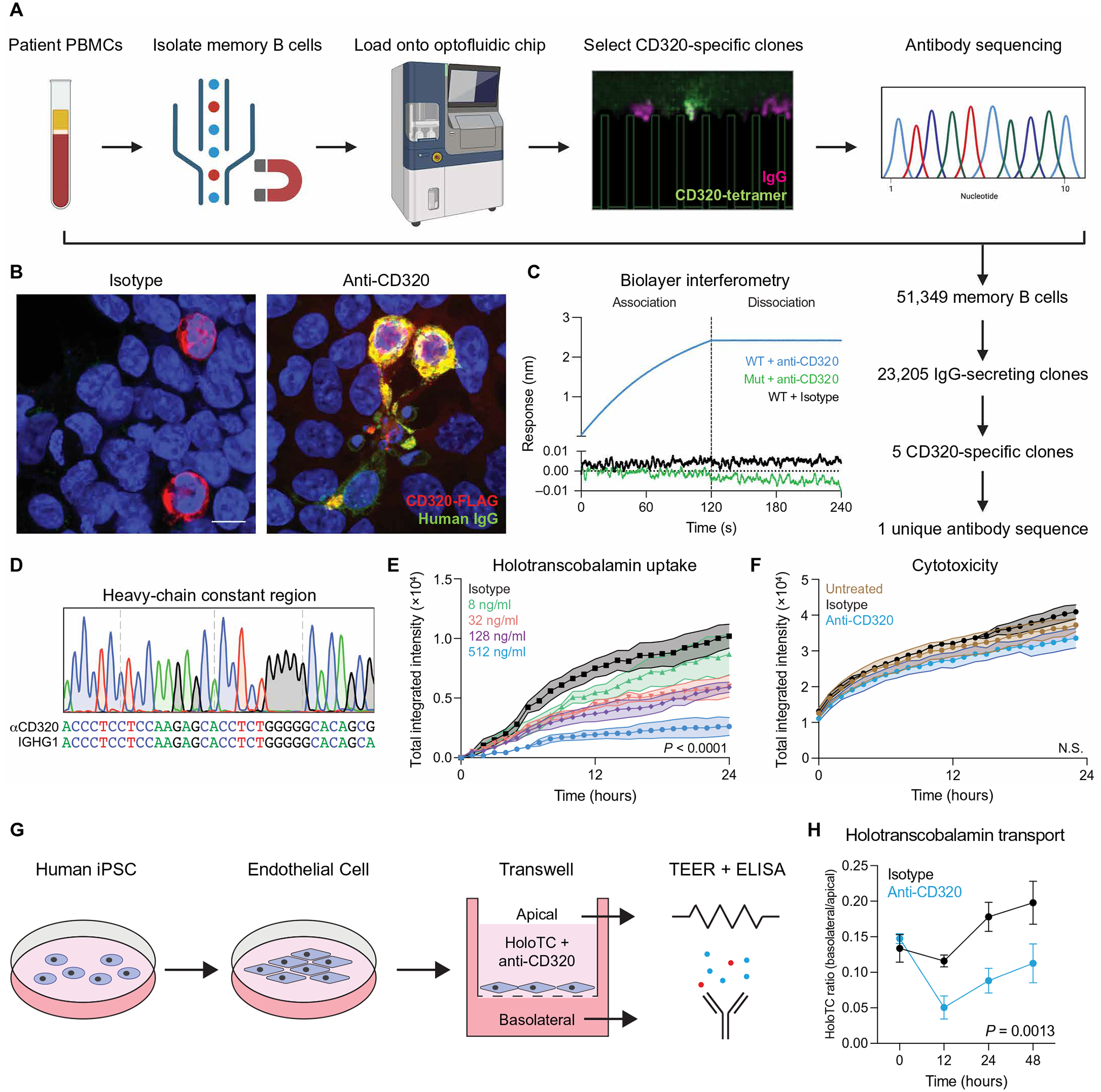
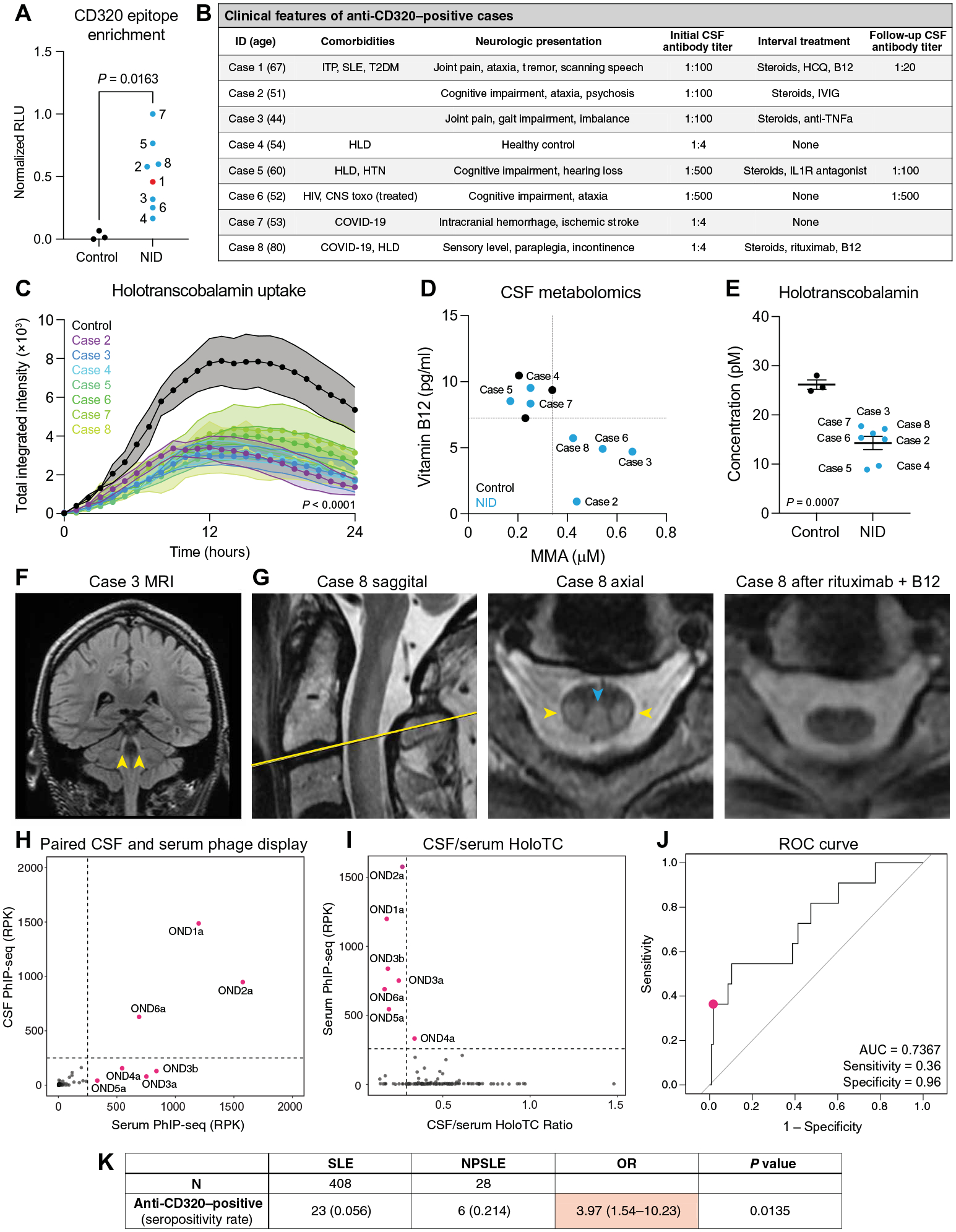
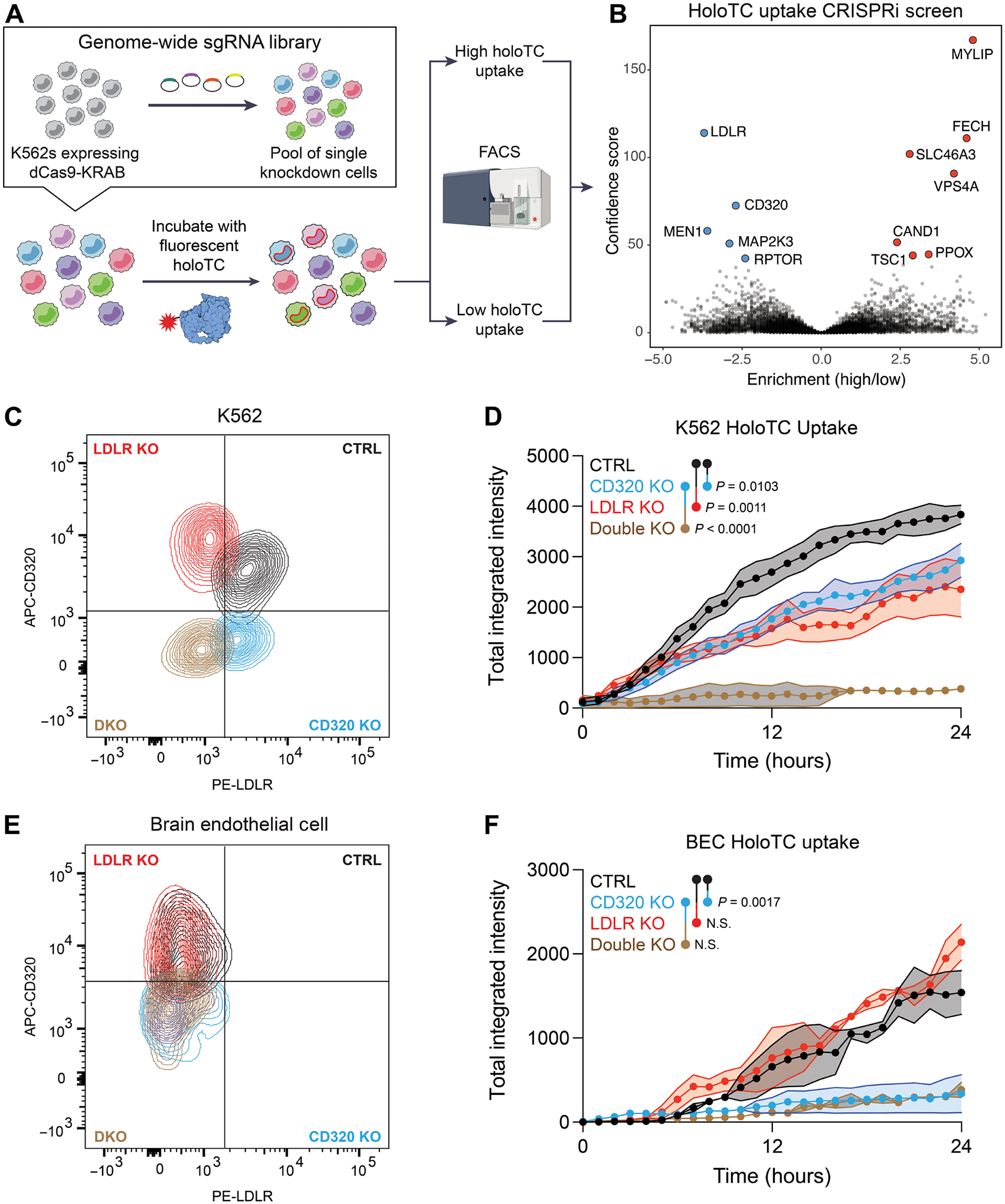
Vitamin B12 is critical for hematopoiesis and myelination. Deficiency can cause neurologic deficits including loss of coordination and cognitive decline. However, diagnosis relies on measurement of vitamin B12 in the blood, which may not accurately reflect the concentration in the brain. Using programmable phage display, we identified an autoantibody targeting the transcobalamin receptor (CD320) in a patient with progressive tremor, ataxia, and scanning speech. Anti-CD320 impaired cellular uptake of cobalamin (B12) in vitro by depleting its target from the cell surface. Despite a normal serum concentration, B12 was nearly undetectable in her cerebrospinal fluid (CSF). Immunosuppressive treatment and high-dose systemic B12 supplementation were associated with increased B12 in the CSF and clinical improvement. Optofluidic screening enabled isolation of a patient-derived monoclonal antibody that impaired B12 transport across an in vitro model of the blood-brain barrier (BBB). Autoantibodies targeting the same epitope of CD320 were identified in seven other patients with neurologic deficits of unknown etiology, 6% of healthy controls, and 21.4% of a cohort of patients with neuropsychiatric lupus. In 132 paired serum and CSF samples, detection of anti-CD320 in the blood predicted B12 deficiency in the brain. However, these individuals did not display any hematologic signs of B12 deficiency despite systemic CD320 impairment. Using a genome-wide CRISPR screen, we found that the low-density lipoprotein receptor serves as an alternative B12 uptake pathway in hematopoietic cells. These findings dissect the tissue specificity of B12 transport and elucidate an autoimmune neurologic condition that may be amenable to immunomodulatory treatment and nutritional supplementation.
Conflict of interest statement
J.V.P., J.L.D., S.J.P., and M.R.W. are coinventors on a patent application related to this work (PCT/US2024/018105, “Compositions and methods related to transcobalamin receptor autoantibodies”). M.R.W. receives unrelated research grant funding from Roche/Genentech and Novartis; received speaking honoraria from Genentech, Takeda, WebMD, and Novartis; and is a founder and paid consultant for Delve Bio Inc. J.L.D. is a founder and paid consultant for Delve Bio Inc. and a paid consultant for the Public Health Company and Allen & Co. M.R.W. and J.L.D. receive licensing fees from CDI Laboratories. C.M.B. is a physician consultant for the Neuroimmune Foundation. J.M.G. receives research support from Hoffman LaRoche and Vigil Neurosciences for clinical trials and is a paid consultant for Arialys and Ventyx Bio. S.L.H. currently serves on the scientific advisory board of Accure, Alector, and Annexon; has previously consulted for BD, Moderna, NGM Bio, and Pheno Therapeutics; previously served on the board of directors of Neurona; and has received travel reimbursement and writing support from F. Hoffmann-La Roche and Novartis AG for anti-CD20 therapy–related meetings and presentations. A.J.G. is an Associate Editor for JAMA Neurology and received advisory board fees from Pipeline Therapeutics outside the submitted work. J.Y. has received grant support from Gilead, Aurinia, and BMS Foundation and performed consulting for Astra Zeneca, Pfizer, and UBC. The other authors declare that they have no competing interests.
Figures
References
-
- Green R, Allen LH, Bjørke-Monsen A-L, Brito A, Guéant J-L, Miller JW, Molloy AM, Nexo E, Stabler S, Toh B-H, Ueland PM, Yajnik C, Vitamin B12 deficiency. Nat. Rev. Dis. Primers 3, 17040 (2017). - PubMed
-
- Stabler SP, Vitamin B12 deficiency. N. Engl. J. Med 368, 149–160 (2013). - PubMed
-
- Hooshmand B, Appold F, Fissler P, Perneczky R, Otto M, Tumani H, Kivipelto M, von Arnim CAF, Markers of vitamin B12 status in relation to cerebrospinal fluid biomarkers of Alzheimer’s disease and cognitive performance. Ann. Neurol 94, 223–231 (2023). - PubMed
-
- Oki R, Izumi Y, Fujita K, Miyamoto R, Nodera H, Sato Y, Sakaguchi S, Nokihara H, Kanai K, Tsunemi T, Hattori N, Hatanaka Y, Sonoo M, Atsuta N, Sobue G, Shimizu T, Shibuya K, Ikeda K, Kano O, Nishinaka K, Kojima Y, Oda M, Komai K, Kikuchi H, Kohara N, Urushitani M, Nakayama Y, Ito H, Nagai M, Nishiyama K, Kuzume D, Shimohama S, Shimohata T, Abe K, Ishihara T, Onodera O, Isose S, Araki N, Morita M, Noda K, Toda T, Maruyama H, Furuya H, Teramukai S, Kagimura T, Noma K, Yanagawa H, Kuwabara S, Kaji R, Efficacy and safety of ultrahigh-dose methylcobalamin in early-stage amyotrophic lateral sclerosis. JAMA Neurol 79, 575–583 (2022). - PMC - PubMed
