

Video analysis of real-life shoulder dystocia to assess technical and non-technical performance
- PMID: 38925557
- PMCID: PMC11426221
- DOI: 10.1111/aogs.14900
Video analysis of real-life shoulder dystocia to assess technical and non-technical performance
Abstract
Introduction: Managing obstetric shoulder dystocia requires swift action using correct maneuvers. However, knowledge of obstetric teams' performance during management of real-life shoulder dystocia is limited, and the impact of non-technical skills has not been adequately evaluated. We aimed to analyze videos of teams managing real-life shoulder dystocia to identify clinical challenges associated with correct management and particular non-technical skills correlated with high technical performance.
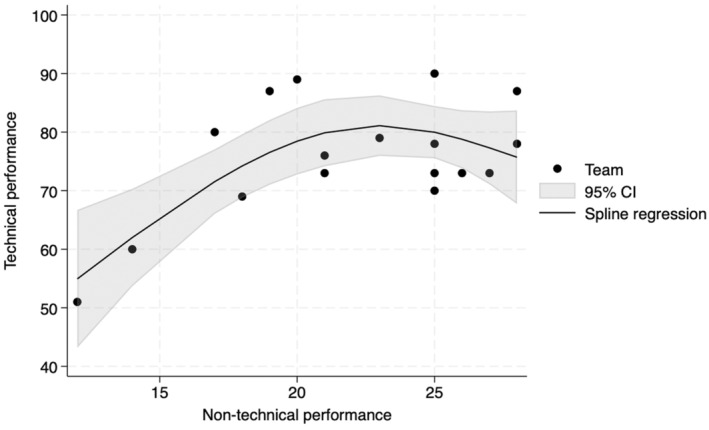
Material and methods: We included 17 videos depicting teams managing shoulder dystocia in two Danish delivery wards, where deliveries were initially handled by midwives, and consultants were available for complications. Delivery rooms contained two or three cameras activated by Bluetooth upon obstetrician entry. Videos were captured 5 min before and after activation. Two obstetricians assessed the videos; technical performances were scored as low (0-59), average (60-84), or high (85-100). Two other assessors evaluated non-technical skills using the Global Assessment of Team Performance checklist, scoring 6 (poor) to 30 (excellent). We used a spline regression model to explore associations between these two score sets. Inter-rater agreement was assessed using interclass correlation coefficients.
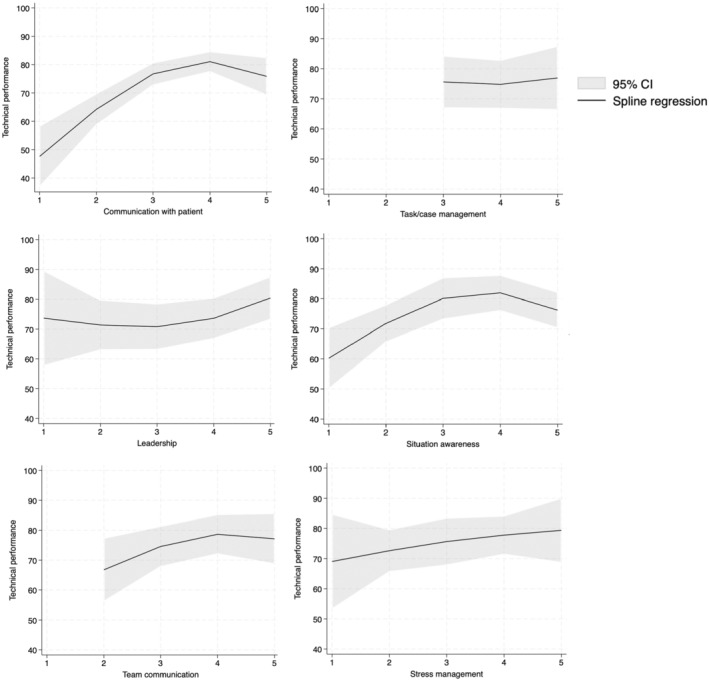
Results: Interclass correlation coefficients were 0.71 (95% confidence interval 0.23-0.89) and 0.82 (95% confidence interval 0.52-0.94) for clinical and non-technical performances, respectively. Two teams had low technical performance scores; four teams achieved high scores. Teams adhered well to guidelines, demonstrating limited head traction, McRoberts maneuver, and internal rotation maneuvers. Several clinical skills posed challenges, notably recognizing shoulder impaction, applying suprapubic pressure, and discouraging women from pushing. Two non-technical skills were associated with high technical performance: effective patient communication, with teams calming the mother and guiding her collaboration during internal rotational maneuvers, and situation awareness, where teams promptly mobilized all essential personnel (senior midwife, consultant, pediatric team). Team communication, stress management, and task management skills were not associated with high technical performance.
Conclusions: Videos capturing teams managing real-life shoulder dystocia are an effective tool to reveal challenges with certain technical and non-technical skills. Teams with high technical performance are associated with effective patient communication and situational awareness. Future training should include technical skills and non-technical skills, patient communication, and situation awareness.
Keywords: checklist; communication; emergency treatment; obstetric labor complications; obstetrics; shoulder dystocia; situation awareness; video recording.
© 2024 The Author(s). Acta Obstetricia et Gynecologica Scandinavica published by John Wiley & Sons Ltd on behalf of Nordic Federation of Societies of Obstetrics and Gynecology (NFOG).
Conflict of interest statement
The authors report no conflicts of interest.
Figures
Similar articles
-
The importance of non-technical performance for teams managing postpartum haemorrhage: video review of 99 obstetric teams.BJOG. 2019 Jul;126(8):1015-1023. doi: 10.1111/1471-0528.15655. Epub 2019 Mar 27. BJOG. 2019. PMID: 30771263 Review.
-
A critical evaluation of the external and internal maneuvers for resolution of shoulder dystocia.Am J Obstet Gynecol. 2024 Mar;230(3S):S1027-S1043. doi: 10.1016/j.ajog.2023.01.016. Epub 2023 Aug 17. Am J Obstet Gynecol. 2024. PMID: 37652778 Review.
-
Team performance during vacuum-assisted vaginal delivery: video review of obstetric multidisciplinary teams.Front Med (Lausanne). 2024 Mar 20;11:1330457. doi: 10.3389/fmed.2024.1330457. eCollection 2024. Front Med (Lausanne). 2024. PMID: 38572162 Free PMC article.
-
Teamwork and Adherence to Guideline on Newborn Resuscitation-Video Review of Neonatal Interdisciplinary Teams.Front Pediatr. 2022 Feb 21;10:828297. doi: 10.3389/fped.2022.828297. eCollection 2022. Front Pediatr. 2022. PMID: 35265565 Free PMC article.
-
Shoulder Dystocia: Managing an Obstetric Emergency.Am Fam Physician. 2020 Jul 15;102(2):84-90. Am Fam Physician. 2020. PMID: 32667171
Cited by
-
Shoulder dystocia-Still a feared complication. How can we improve?Acta Obstet Gynecol Scand. 2024 Oct;103(10):1908-1909. doi: 10.1111/aogs.14952. Epub 2024 Aug 22. Acta Obstet Gynecol Scand. 2024. PMID: 39171555 Free PMC article. No abstract available.
References
-
- Crofts J, Draycott T, Montague I, Winter C, Fox R. Shoulder dystocia. Green–top Guideline No. 42. 2nd ed. 2012.
-
- Practice bulletin No 178: shoulder dystocia. Obstet Gynecol. 2017;129:e123‐e133. - PubMed
-
- Gherman RB, Ouzounian JG, Goodwin TM. Obstetric maneuvers for shoulder dystocia and associated fetal morbidity. Am J Obstet Gynecol. 1998;178:1126‐1130. - PubMed
-
- Gherman RB, Chauhan S, Ouzounian JG, Lerner H, Gonik B, Goodwin TM. Shoulder dystocia: the unpreventable obstetric emergency with empiric management guidelines. Am J Obstet Gynecol. 2006;195:657‐672. - PubMed
-
- Draycott TJ, Crofts JF, Ash JP, et al. Improving neonatal outcome through practical shoulder dystocia training. Obstet Gynecol. 2008;112:14‐20. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
