

SGLT-2 inhibitors, GLP-1 receptor agonists, and DPP-4 inhibitors and risk of hyperkalemia among people with type 2 diabetes in clinical practice: population based cohort study
- PMID: 38925801
- PMCID: PMC11200155
- DOI: 10.1136/bmj-2023-078483
SGLT-2 inhibitors, GLP-1 receptor agonists, and DPP-4 inhibitors and risk of hyperkalemia among people with type 2 diabetes in clinical practice: population based cohort study
Abstract
Objectives: To evaluate the comparative effectiveness of sodium-glucose cotransporter-2 (SGLT-2) inhibitors, glucagon-like peptide-1 (GLP-1) receptor agonists, and dipeptidyl peptidase-4 (DPP-4) inhibitors in preventing hyperkalemia in people with type 2 diabetes in routine clinical practice.
Design: Population based cohort study with active-comparator, new user design.
Setting: Claims data from Medicare and two large commercial insurance databases in the United States from April 2013 to April 2022.
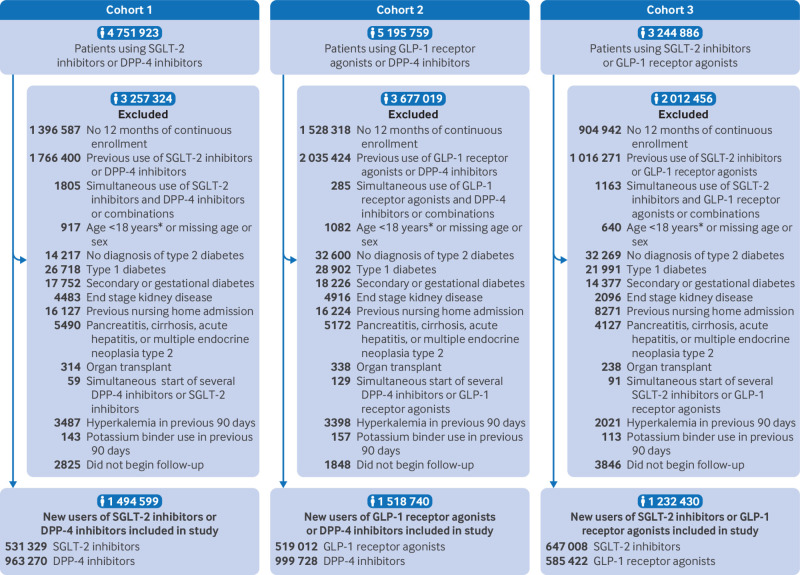
Participants: 1:1 propensity score matched adults with type 2 diabetes newly starting SGLT-2 inhibitors versus DPP-4 inhibitors (n=778 908), GLP-1 receptor agonists versus DPP-4 inhibitors (n=729 820), and SGLT-2 inhibitors versus GLP-1 receptor agonists (n=873 460).
Main outcome measures: Hyperkalemia diagnosis in the inpatient or outpatient setting. Secondary outcomes were hyperkalemia defined as serum potassium levels ≥5.5 mmol/L and hyperkalemia diagnosis in the inpatient or emergency department setting.
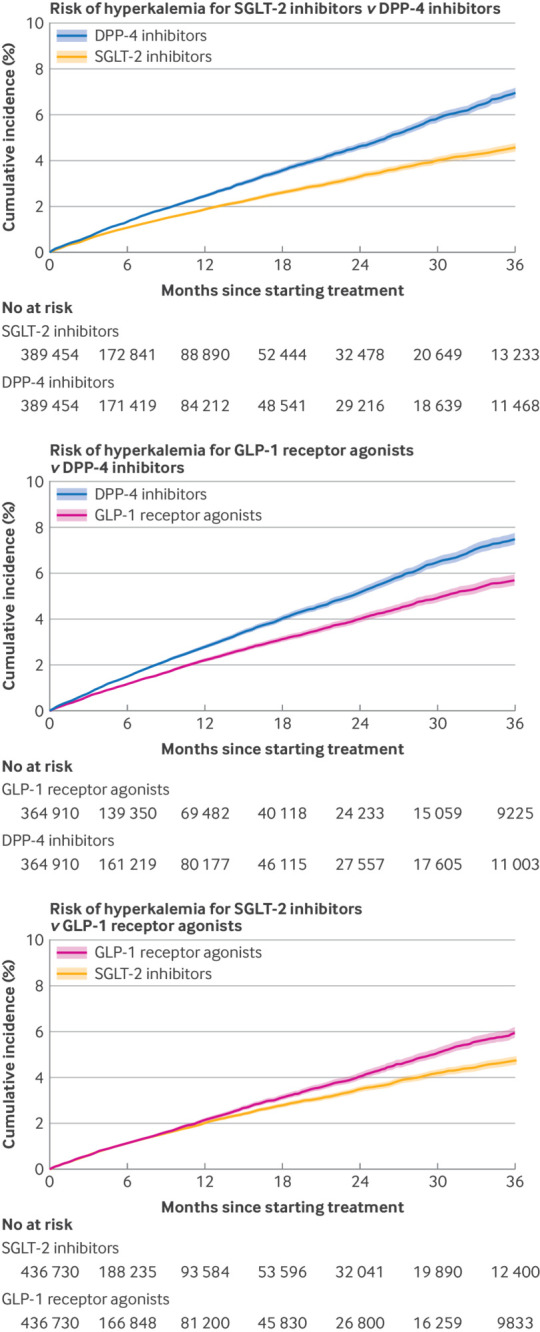
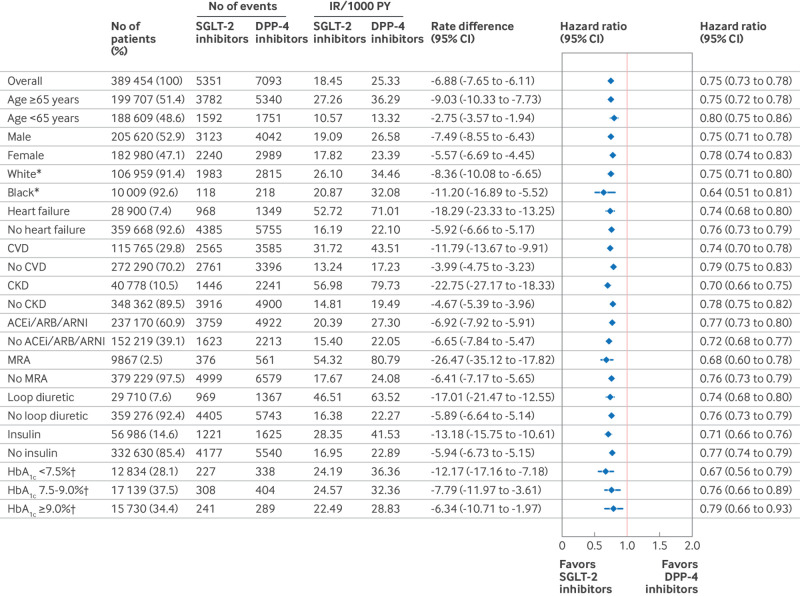
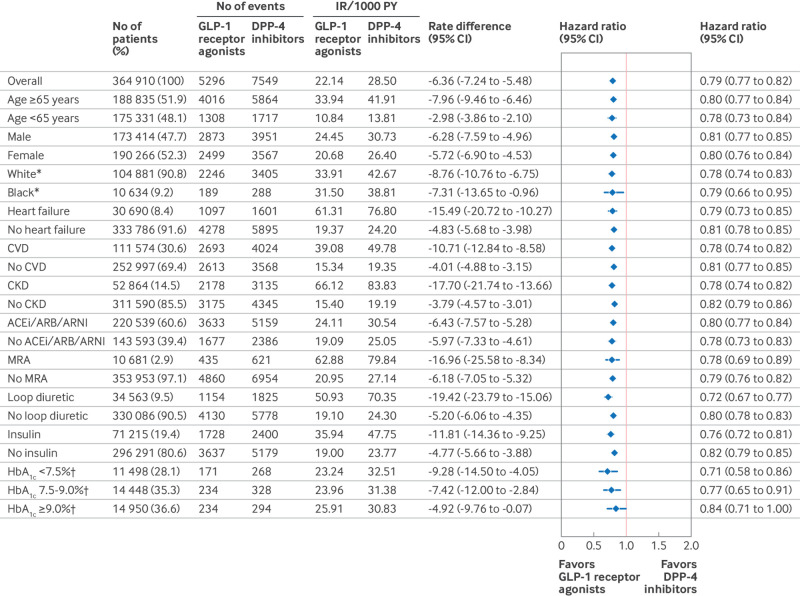
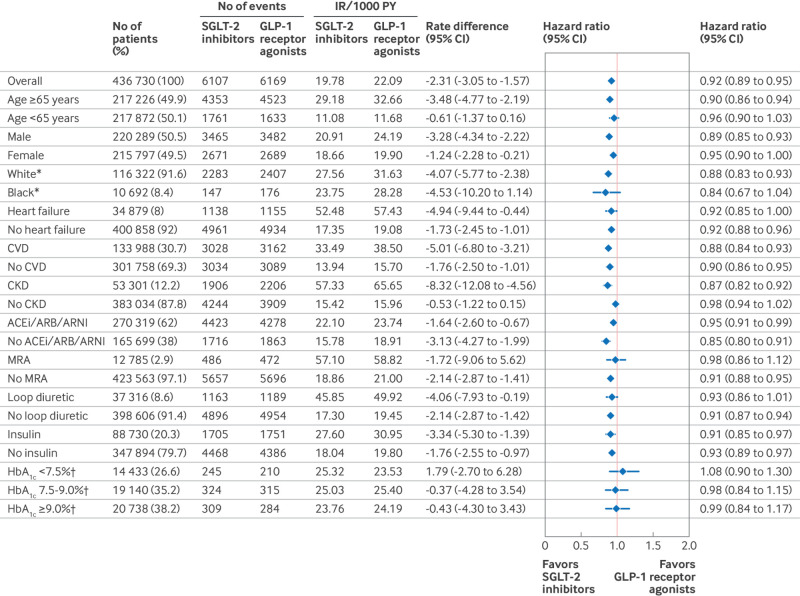
Results: Starting SGLT-2 inhibitor treatment was associated with a lower rate of hyperkalemia than DPP-4 inhibitor treatment (hazard ratio 0.75, 95% confidence interval (CI) 0.73 to 0.78) and a slight reduction in rate compared with GLP-1 receptor agonists (0.92, 0.89 to 0.95). Use of GLP-1 receptor agonists was associated with a lower rate of hyperkalemia than DPP-4 inhibitors (0.79, 0.77 to 0.82). The three year absolute risk was 2.4% (95% CI 2.1% to 2.7%) lower for SGLT-2 inhibitors than DPP-4 inhibitors (4.6% v 7.0%), 1.8% (1.4% to 2.1%) lower for GLP-1 receptor agonists than DPP-4 inhibitors (5.7% v 7.5%), and 1.2% (0.9% to 1.5%) lower for SGLT-2 inhibitors than GLP-1 receptor agonists (4.7% v 6.0%). Findings were consistent for the secondary outcomes and among subgroups defined by age, sex, race, medical conditions, other drug use, and hemoglobin A1c levels on the relative scale. Benefits for SGLT-2 inhibitors and GLP-1 receptor agonists on the absolute scale were largest for those with heart failure, chronic kidney disease, or those using mineralocorticoid receptor antagonists. Compared with DPP-4 inhibitors, the lower rate of hyperkalemia was consistently observed across individual agents in the SGLT-2 inhibitor (canagliflozin, dapagliflozin, empagliflozin) and GLP-1 receptor agonist (dulaglutide, exenatide, liraglutide, semaglutide) classes.
Conclusions: In people with type 2 diabetes, SGLT-2 inhibitors and GLP-1 receptor agonists were associated with a lower risk of hyperkalemia than DPP-4 inhibitors in the overall population and across relevant subgroups. The consistency of associations among individual agents in the SGLT-2 inhibitor and GLP-1 receptor agonist classes suggests a class effect. These ancillary benefits of SGLT-2 inhibitors and GLP-1 receptor agonists further support their use in people with type 2 diabetes, especially in those at risk of hyperkalemia.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest/ and declare the following: support from Brigham and Women’s Hospital, Harvard Medical School, the Netherlands Organization for Scientific Research, Patient-Centered Outcomes Research Institute, Food and Drug Administration, National Institutes of Health, National Institute on Aging, American Diabetes Association for the submitted work. EP is principal investigator of an investigator initiated grant to the Brigham and Women’s Hospital from Boehringer Ingelheim, not directly related to the topic of the submitted work; DJW reports serving on data monitoring committees for Novo Nordisk not related to the topic of this work; SJC reports serving on advisory boards for Alexion Pharmaceuticals and employment of a family member by a Johnson and Johnson company. No other potential conflicts of interest relevant to this article were reported.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous