

Use of ketamine in Super Refractory Status Epilepticus: a systematic review
- PMID: 38926769
- PMCID: PMC11210084
- DOI: 10.1186/s42466-024-00322-7
Use of ketamine in Super Refractory Status Epilepticus: a systematic review
Erratum in
-
Correction: Use of ketamine in super refractory status epilepticus: a systematic review.Neurol Res Pract. 2024 Jul 9;6(1):38. doi: 10.1186/s42466-024-00335-2. Neurol Res Pract. 2024. PMID: 38978102 Free PMC article. No abstract available.
Abstract
Objective: This review specifically investigates ketamine's role in SRSE management.
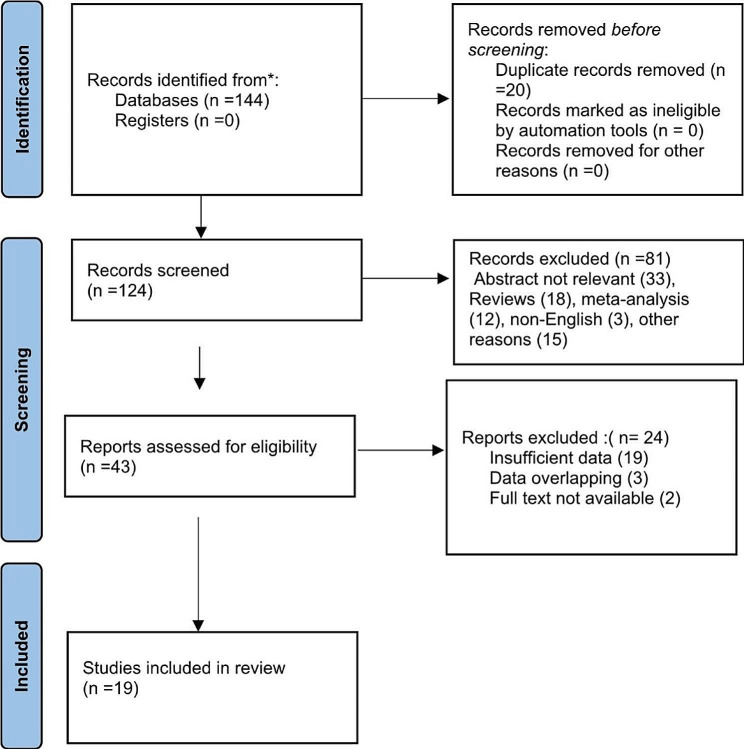
Methods: PubMed, EMBASE, and Google Scholar databases were searched from inception to May 1st, 2023, for English-language literature. Inclusion criteria encompassed studies on SRSE in humans of all ages and genders treated with ketamine.
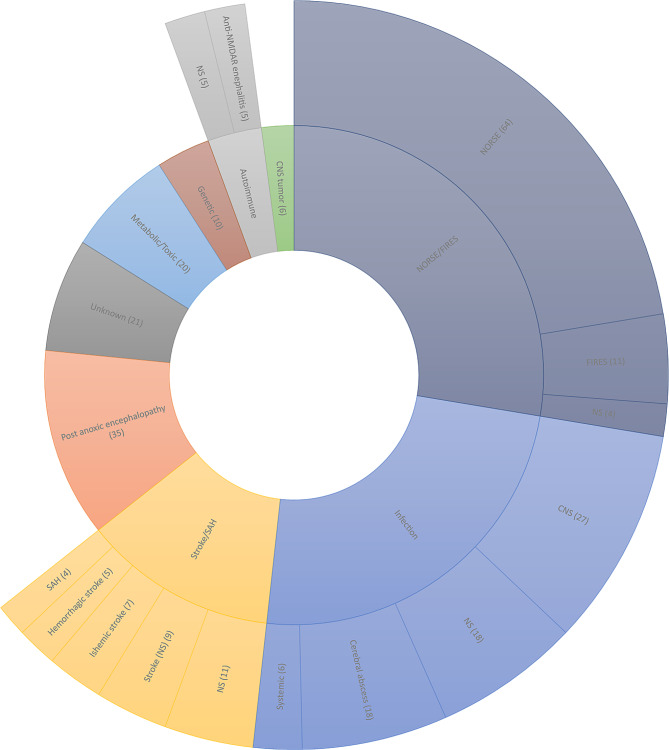
Results: In this systematic review encompassing 19 studies with 336 participants, age ranged from 9 months to 86 years. Infections, anoxia, and metabolic issues emerged as the common causes of SRSE, while some cases had unknown origins, termed as NORSE (New Onset RSE) or FIRESs (Febrile Infection-Related Epilepsy Syndrome). Most studies categorized SRSE cases into convulsive (N = 105) and non-convulsive (N = 197). Ketamine was used after failed antiepileptics and anesthetics in 17 studies, while in others, it was a first or second line of treatment. Dosages varied from 0.5 mg/kg (bolus) and 0.2-15 mg/kg/hour (maintenance) in adults and 1-3 mg/kg (bolus) and 0.5-3 mg/kg/hour (maintenance) in pediatrics, lasting one to 30 days. Ketamine was concurrently used with other drugs in 40-100% of cases, most frequently propofol and midazolam. Seizure resolution rate varied from 53.3 to 91% and 40-100% in larger (N = 42-68) and smaller case series (N = 5-20) respectively. Seizure resolution occurred in every case of case report except in one in which the patient died. Burst suppression in EEG was reported in 12 patients from two case series and two case reports. Recurrence was reported in 11 patients from five studies. The reported all-cause mortality varied from 38.8 to 59.5% and 0-36.4% in larger and smaller case series., unrelated directly to ketamine dosage or duration.
Significance: Ketamine demonstrates safety and effectiveness in SRSE, offering advantages over GABAergic drugs by acting on NMDA receptors, providing neuroprotection, and reducing vasopressor requirement.
Keywords: Burst suppression; Convulsive Status Epilepticus (CSE); NMDA agonist; Neuroprotection; Non-convulsive Status Epilepticus (NCSE); SRSE; STESS score.
© 2024. The Author(s).
Conflict of interest statement
None of the authors has any conflict of interest to disclose.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources