

Multidisciplinary Perspectives of Challenges in Infective Endocarditis Complicated by Septic Embolic-Induced Acute Myocardial Infarction
- PMID: 38927180
- PMCID: PMC11201065
- DOI: 10.3390/antibiotics13060513
Multidisciplinary Perspectives of Challenges in Infective Endocarditis Complicated by Septic Embolic-Induced Acute Myocardial Infarction
Abstract
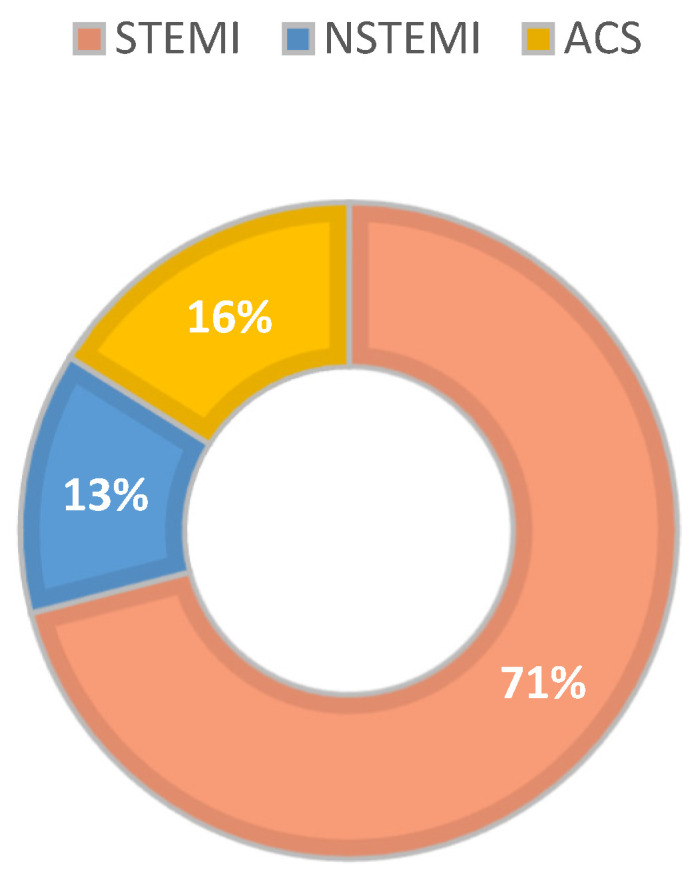
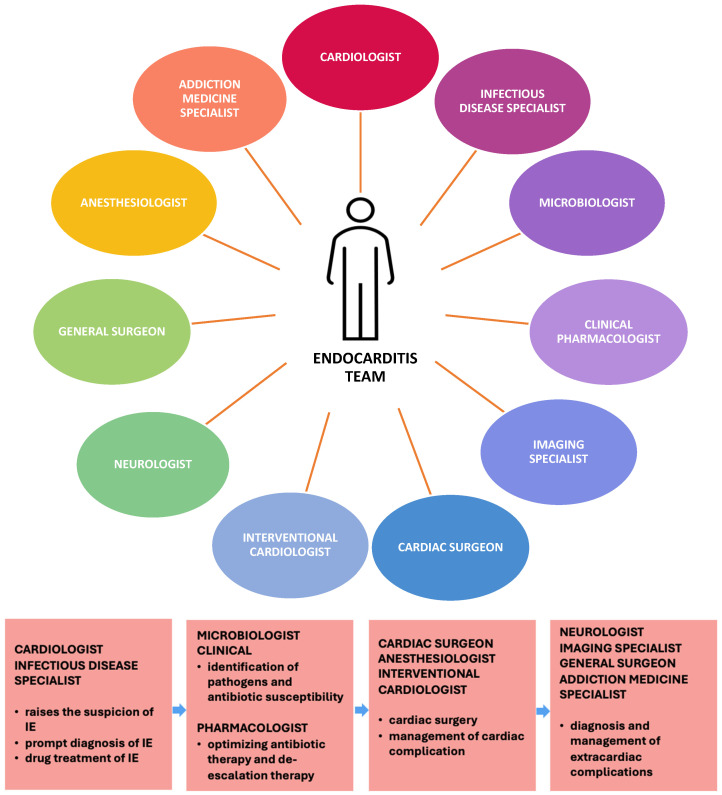
Background: Infective endocarditis (IE) management is challenging, usually requiring multidisciplinary collaboration from cardiologists, infectious disease specialists, interventional cardiologists, and cardiovascular surgeons, as more than half of the cases will require surgical procedures. Therefore, it is essential for all healthcare providers involved in managing IE to understand the disease's characteristics, potential complications, and treatment options. While systemic embolization is one of the most frequent complications of IE, the coronary localization of emboli causing acute myocardial infarction (AMI) is less common, with an incidence ranging from 1% to 10% of cases, but it has a much higher rate of morbidity and mortality. There are no guidelines for this type of AMI management in IE.
Methods: This narrative review summarizes the current knowledge regarding septic coronary embolization in patients with IE. Additionally, this paper highlights the diagnosis and management challenges in such cases, particularly due to the lack of protocols or consensus in the field.
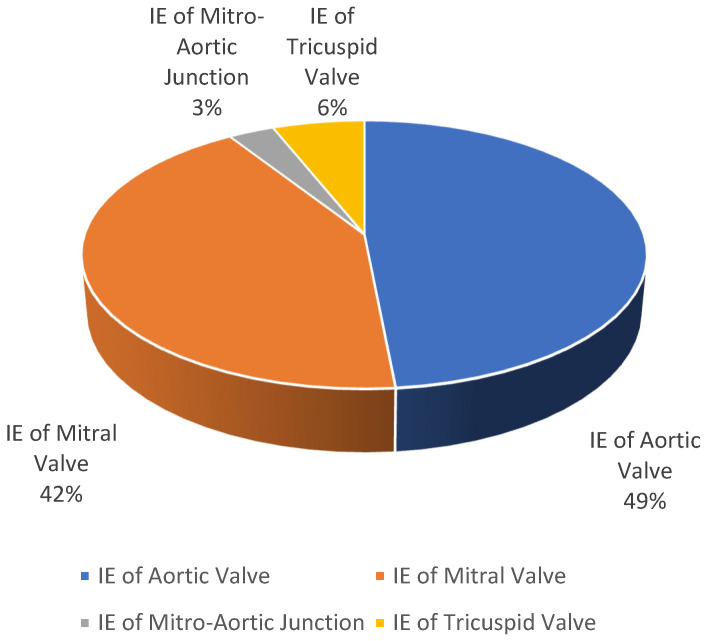
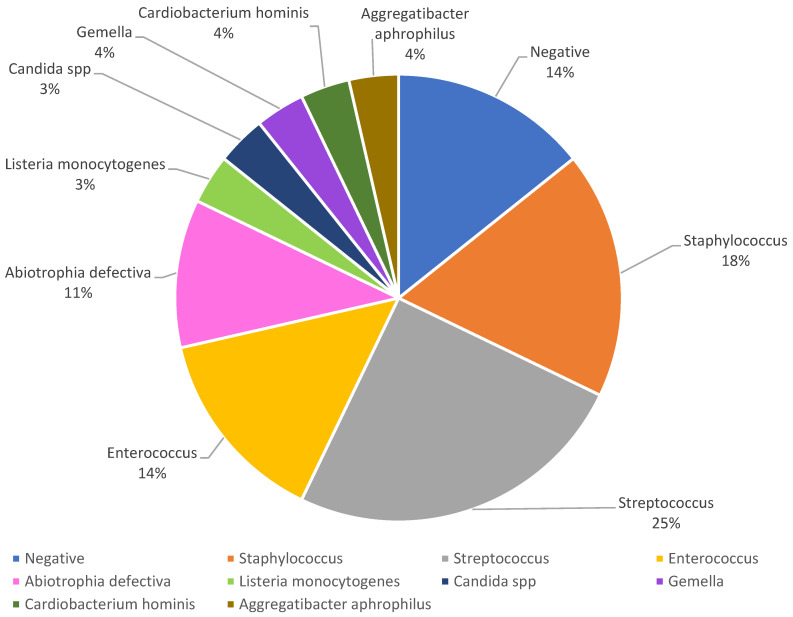
Results: Data extracted from case reports indicate that septic coronary embolization often occurs within the first two weeks of the disease. The aortic valve is most commonly involved with vegetation, and the occluded vessel is frequently the left anterior descending artery. Broad-spectrum antibiotic therapy followed by targeted antibiotic therapy for infection control is essential, and surgical treatment offers promising results through surgical embolectomy, concomitant with valve replacement or aspiration thrombectomy, with or without subsequent stent insertion. Thrombolytics are to be avoided due to the increased risk of bleeding.
Conclusions: All these aspects should constitute future lines of research, allowing the integration of all current knowledge from multidisciplinary team studies on larger patient cohorts and, subsequently, creating a consensus for assessing the risk and guiding the management of this potentially fatal complication.
Keywords: antibiotic therapy; coronary; endocarditis; myocardial infarction; septic embolism.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Momtazmanesh S., Saeedi Moghaddam S., Malakan Rad E., Azadnajafabad S., Ebrahimi N., Mohammadi E., Rouhifard M., Rezaei N., Masinaei M., Rezaei N., et al. Global, Regional, and National Burden and Quality of Care Index of Endocarditis: The Global Burden of Disease Study 1990–2019. Eur. J. Prev. Cardiol. 2022;29:1287–1297. doi: 10.1093/eurjpc/zwab211. - DOI - PubMed
-
- Cabezón G., López J., Vilacosta I., Sáez C., García-Granja P.E., Olmos C., Jerónimo A., Gutiérrez Á., Pulido P., de Miguel M., et al. Reassessment of Vegetation Size as a Sole Indication for Surgery in Left-Sided Infective Endocarditis. J. Am. Soc. Echocardiogr. 2022;35:570–575. doi: 10.1016/j.echo.2021.12.013. - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
