

Design and Evaluation of ScanCap: A Low-Cost, Reusable Tethered Capsule Endoscope with Blue-Green Illumination Imaging for Unsedated Screening and Early Detection of Barrett's Esophagus
- PMID: 38927792
- PMCID: PMC11200367
- DOI: 10.3390/bioengineering11060557
Design and Evaluation of ScanCap: A Low-Cost, Reusable Tethered Capsule Endoscope with Blue-Green Illumination Imaging for Unsedated Screening and Early Detection of Barrett's Esophagus
Abstract
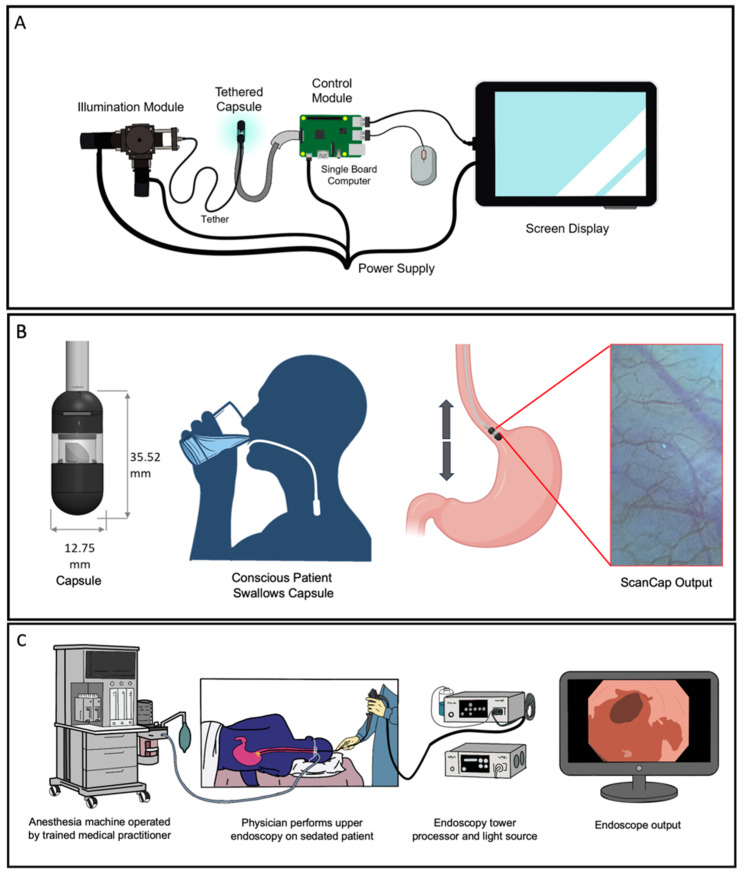
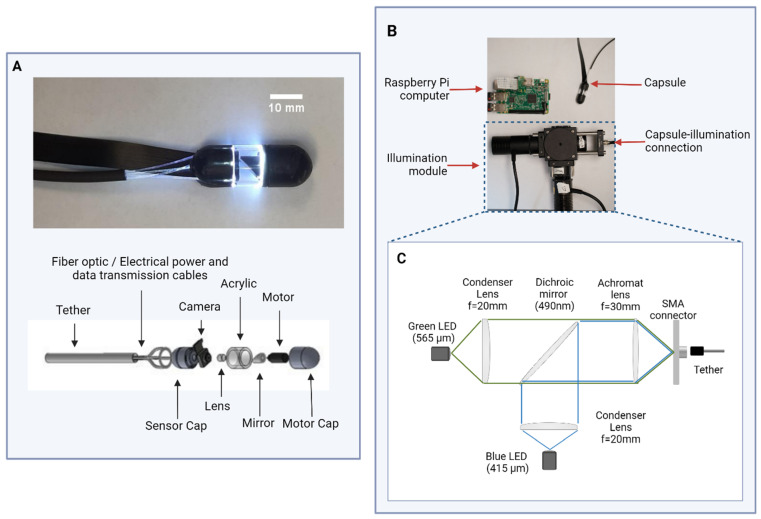
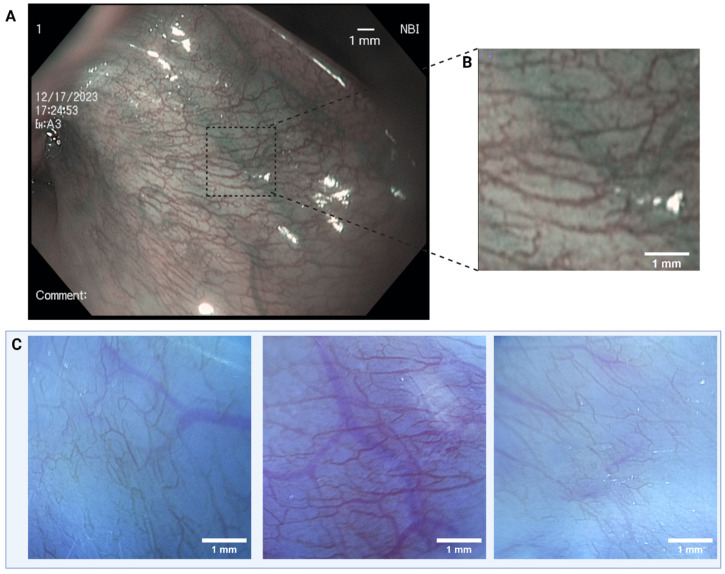
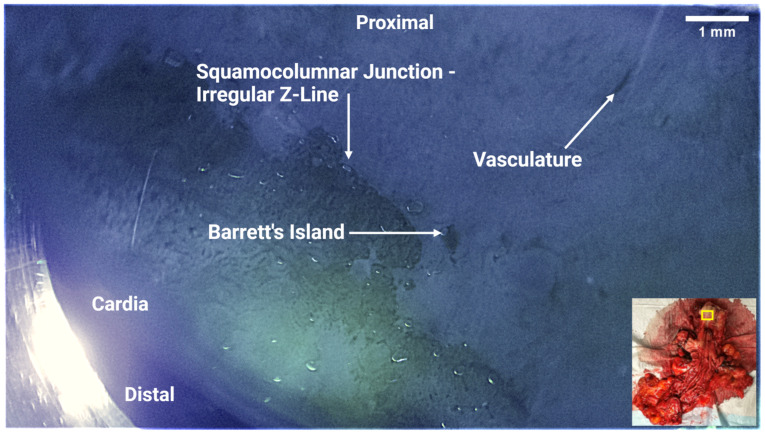
Esophageal carcinoma is the sixth-leading cause of cancer death worldwide. A precursor to esophageal adenocarcinoma (EAC) is Barrett's Esophagus (BE). Early-stage diagnosis and treatment of esophageal neoplasia (Barrett's with high-grade dysplasia/intramucosal cancer) increase the five-year survival rate from 10% to 98%. BE is a global challenge; however, current endoscopes for early BE detection are costly and require extensive infrastructure for patient examination and sedation. We describe the design and evaluation of the first prototype of ScanCap, a high-resolution optical endoscopy system with a reusable, low-cost tethered capsule, designed to provide high-definition, blue-green illumination imaging for the early detection of BE in unsedated patients. The tethered capsule (12.8 mm diameter, 35.5 mm length) contains a color camera and rotating mirror and is designed to be swallowed; images are collected as the capsule is retracted manually via the tether. The tether provides electrical power and illumination at wavelengths of 415 nm and 565 nm and transmits data from the camera to a tablet. The ScanCap prototype capsule was used to image the oral mucosa in normal volunteers and ex vivo esophageal resections; images were compared to those obtained using an Olympus CV-180 endoscope. Images of superficial capillaries in intact oral mucosa were clearly visible in ScanCap images. Diagnostically relevant features of BE, including irregular Z-lines, distorted mucosa, and dilated vasculature, were clearly visible in ScanCap images of ex vivo esophageal specimens.
Keywords: Barrett’s esophagus; cancer detection; cancer screening; capsule endoscopy; digital chromoendoscopy; esophageal cancer; global health; low-resource settings; narrow-band imaging.
Conflict of interest statement
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures

References
Grants and funding
LinkOut - more resources
Full Text Sources
