

Development of a Simple Scoring System for Predicting Discharge Safety from the Medical ICU to Low-Acuity Wards: The Role of the Sequential Organ Failure Assessment Score, Albumin, and Red Blood Cell Distribution Width
- PMID: 38929864
- PMCID: PMC11204447
- DOI: 10.3390/jpm14060643
Development of a Simple Scoring System for Predicting Discharge Safety from the Medical ICU to Low-Acuity Wards: The Role of the Sequential Organ Failure Assessment Score, Albumin, and Red Blood Cell Distribution Width
Abstract
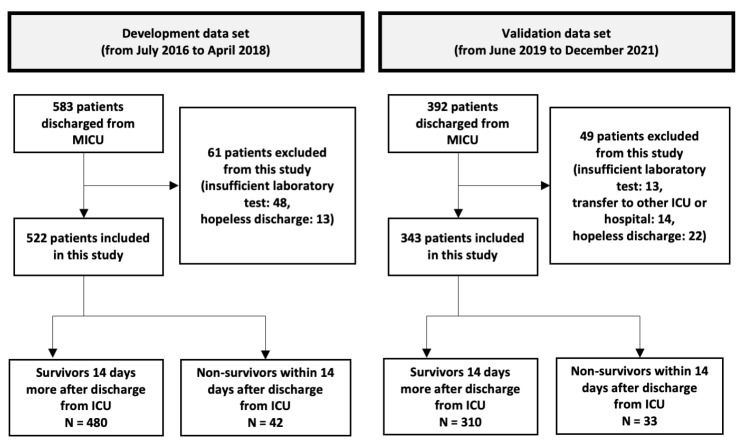
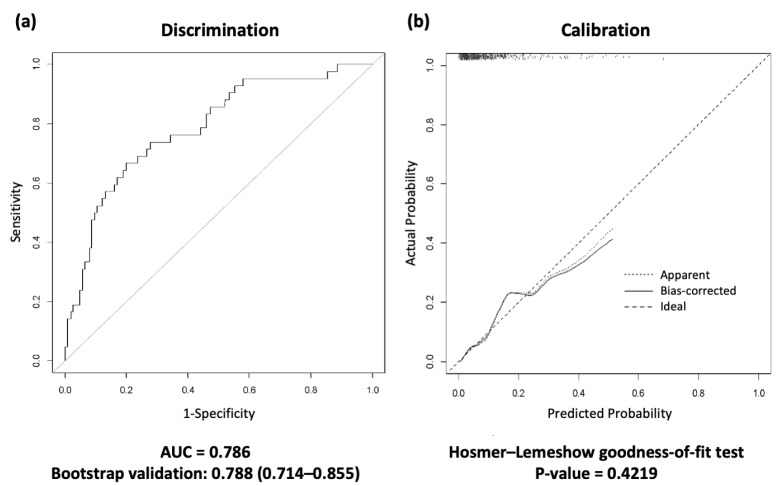
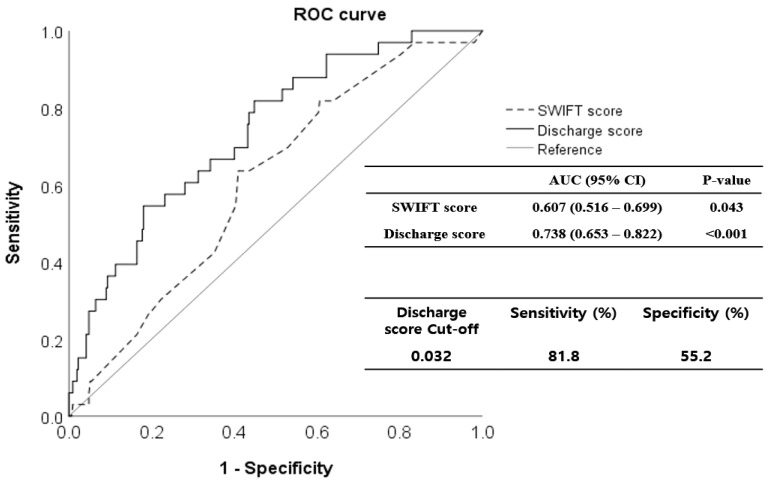
Despite advancements in artificial intelligence-based decision-making, transitioning patients from intensive care units (ICUs) to low-acuity wards is challenging, especially in resource-limited settings. This study aimed to develop a simple scoring system to predict ICU discharge safety. We retrospectively analyzed patients admitted to a tertiary hospital's medical ICU (MICU) between July 2016 and December 2021. This period was divided into two phases for model development and validation. We identified risk factors associated with unexpected death within 14 days of MICU discharge and developed a predictive scoring system that incorporated these factors. We verified the system's performance using validation data. In the development cohort, 522 patients were discharged from the MICU, and 42 (8.04%) died unexpectedly. In multivariate analysis, the Sequential Organ Failure Assessment (SOFA) score (odds ratio [OR] 1.26, 95% confidence interval [CI] 1.13-1.41), red blood cell distribution width (RDW) (OR 1.20, 95% CI 1.07-1.36), and albumin (OR 0.37, 95% CI 0.16-0.84) were predictors of unexpected death. Each variable was assigned a weighted point in the scoring system, and the area under the curve (AUC) was 0.788 (95% CI 0.714-0.855). The scoring system was performed using an AUC of 0.738 (95% CI 0.653-0.822) in the validation cohort of 343 patients with 9.62% of unexpected deaths. When a cut-off of 0.032 was applied, a sensitivity and a specificity of 81.8% and 55.2%, respectively, were achieved. This simple bedside predictive score for ICU discharge uses the SOFA score, albumin level, and RDW to aid in timely decision-making and optimize critical care facility allocation in resource-limited settings.
Keywords: SOFA; albumin; discharge; intensive care unit; prediction; red cell distribution width.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
[A new warning scoring system establishment for prediction of sepsis in patients with trauma in intensive care unit].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2019 Apr;31(4):422-427. doi: 10.3760/cma.j.issn.2095-4352.2019.04.010. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2019. PMID: 31109414 Chinese.
-
[Predictive value of six critical illness scores for 28-day death risk in comprehensive and specialized intensive care unit patients based on MIMIC-IV database].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2022 Jul;34(7):752-758. doi: 10.3760/cma.j.cn121430-20220304-00205. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2022. PMID: 36100416 Chinese.
-
[Comparison of four early warning scores in predicting the prognosis of critically ill patients in secondary hospitals].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2023 Oct;35(10):1093-1098. doi: 10.3760/cma.j.cn121430-20230614-00441. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2023. PMID: 37873716 Chinese.
-
Serum procalcitonin level and SOFA score at discharge from the intensive care unit predict post-intensive care unit mortality: a prospective study.PLoS One. 2014 Dec 2;9(12):e114007. doi: 10.1371/journal.pone.0114007. eCollection 2014. PLoS One. 2014. PMID: 25460569 Free PMC article.
-
[Combined prognostic value of serum lactic acid, procalcitonin and severity score for short-term prognosis of septic shock patients].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2021 Mar;33(3):281-285. doi: 10.3760/cma.j.cn121430-20201113-00715. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2021. PMID: 33834968 Chinese.
Cited by
-
Development of a Nomogram for Predicting ICU Readmission.Cureus. 2024 Oct 15;16(10):e71555. doi: 10.7759/cureus.71555. eCollection 2024 Oct. Cureus. 2024. PMID: 39544597 Free PMC article.
References
-
- Azoulay E., Adrie C., De Lassence A., Pochard F., Moreau D., Thiery G., Cheval C., Moine P., Garrouste-Orgeas M., Alberti C., et al. Determinants of postintensive care unit mortality: A prospective multicenter study. Crit. Care Med. 2003;31:428–432. doi: 10.1097/01.Ccm.0000048622.01013.88. - DOI - PubMed
-
- Ranzani O.T., Prada L.F., Zampieri F.G., Battaini L.C., Pinaffi J.V., Setogute Y.C., Salluh J.I., Povoa P., Forte D.N., Azevedo L.C., et al. Failure to reduce C-reactive protein levels more than 25% in the last 24 hours before intensive care unit discharge predicts higher in-hospital mortality: A cohort study. J. Crit. Care. 2012;27:525.e9–525.e15. doi: 10.1016/j.jcrc.2011.10.013. - DOI - PubMed
LinkOut - more resources
Full Text Sources
