

Medication and Outcome in Older Heart Failure Patients: Results from a Prospective Cohort Study
- PMID: 38931378
- PMCID: PMC11206917
- DOI: 10.3390/ph17060711
Medication and Outcome in Older Heart Failure Patients: Results from a Prospective Cohort Study
Abstract
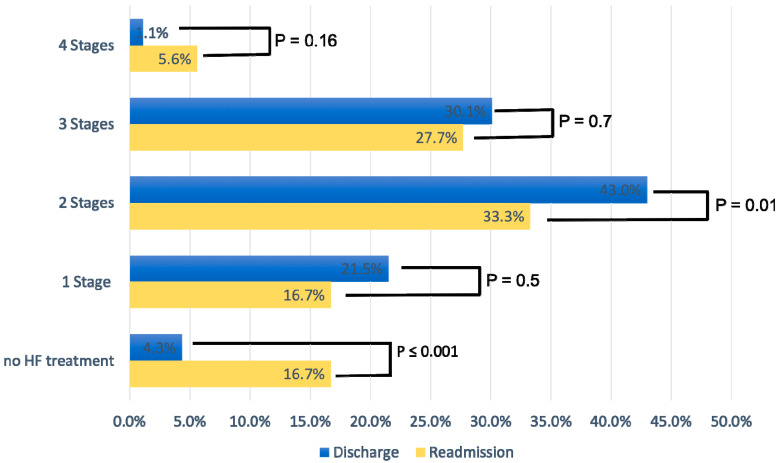
Purpose: Acute heart failure (AHF) is associated with high morbidity and mortality, and the prognosis is particularly poor in older patients. Although the application of guideline-directed medical therapy (GDMT) has shown a positive impact on prognosis, the effects are less clear in older age groups. The aim of this study was to analyze real-world data regarding GDMT and outcomes in older HF patients. Methods: This is a prospective cohort study from a secondary care hospital in central Switzerland. A total of 97 consecutive patients aged ≥60 years were enrolled between January 2019 and 2022. The main outcome parameters were prescribed GDMT at discharge, and in case of rehospitalization, GDMT at readmission, and survival in terms of all-cause mortality and HF-related hospitalizations during a 3-year follow-up period. Results: Follow-up data were available for 93/97 patients. The mean age was 77.8 ± 9.8 years, 46% being female. The mean left ventricular ejection fraction (LVEF) was 35.3 ± 13.9%, with a mean BNP level of 2204.3 ± 239 ng/L. Upon discharge, 86% received beta-blockers and 76.3% received renin-angiotensin system (RAS) inhibitors. At rehospitalization for AHF, beta-blockers use was significantly lower and decreased to 52.8% (p = 0.003), whereas RAS inhibitor use increased slightly to 88.9% (p = 0.07), and SGLT-2 inhibitors showed a significant increase from 5.4% vs. 47.2% (p = 0.04). GDMT prescription was not dependent on LVEF. Overall, 73.1% of patients received two-stage or three-stage GDMT at discharge, whereas this percentage decreased to 61% at rehospitalization (p = 0.01). Kaplan-Meier analysis for the combined outcome rehospitalization and death stratified by LV function showed significant differences between LVEF groups (aHR: 0.6 [95% CI: 0.44 to 0.8]; p = 0.0023). Conclusions: Our results indicate that first, the majority of older AHF patients from a secondary care hospital in Switzerland were not on optimal GDMT at discharge and even fewer at readmission, and second, that prognosis of the population is still poor, with almost half of the patients having been rehospitalized or died during a 3-year follow-up period under real-world conditions, without significant difference between women and men. Our findings underline the need for further improvements in the medical treatment of AHF, in particular in older patients, to improve prognosis and to reduce the burden of disease.
Keywords: heart failure; medical treatment; mortality; older patients; prognosis; rehospitalization.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


References
-
- Conrad N., Judge A., Tran J., Mohseni H., Hedgecott D., Crespillo A.P., Allison M., Hemingway H., Cleland J.G., McMurray J.J.V., et al. Temporal trends and patterns in heart failure incidence: A population-based study of 4 million individuals. Lancet. 2018;391:572–580. doi: 10.1016/S0140-6736(17)32520-5. - DOI - PMC - PubMed
-
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1789–1858. doi: 10.1016/S0140-6736(18)32279-7. Erratum in Lancet 2019, 393, e44. - DOI - PMC - PubMed
-
- Smeets M., Vaes B., Mamouris P., Van Den Akker M., Van Pottelbergh G., Goderis G., Janssens S., Aertgeerts B., Henrard S. Burden of heart failure in Flemish general practices: A registry-based study in the Intego database. BMJ Open. 2019;9:e022972. doi: 10.1136/bmjopen-2018-022972. - DOI - PMC - PubMed
-
- Virani S.S., Alonso A., Benjamin E.J., Bittencourt M.S., Callaway C.W., Carson A.P., Chamberlain A.M., Chang A.R., Cheng S., Delling F.N., et al. Heart Disease and Stroke Statistics-2020 Update: A Report from the American Heart Association. Circulation. 2020;141:e139–e596. doi: 10.1161/CIR.0000000000000757. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
