

Modulation of Brain Cholesterol Metabolism through CYP46A1 Overexpression for Rett Syndrome
- PMID: 38931878
- PMCID: PMC11207948
- DOI: 10.3390/pharmaceutics16060756
Modulation of Brain Cholesterol Metabolism through CYP46A1 Overexpression for Rett Syndrome
Abstract
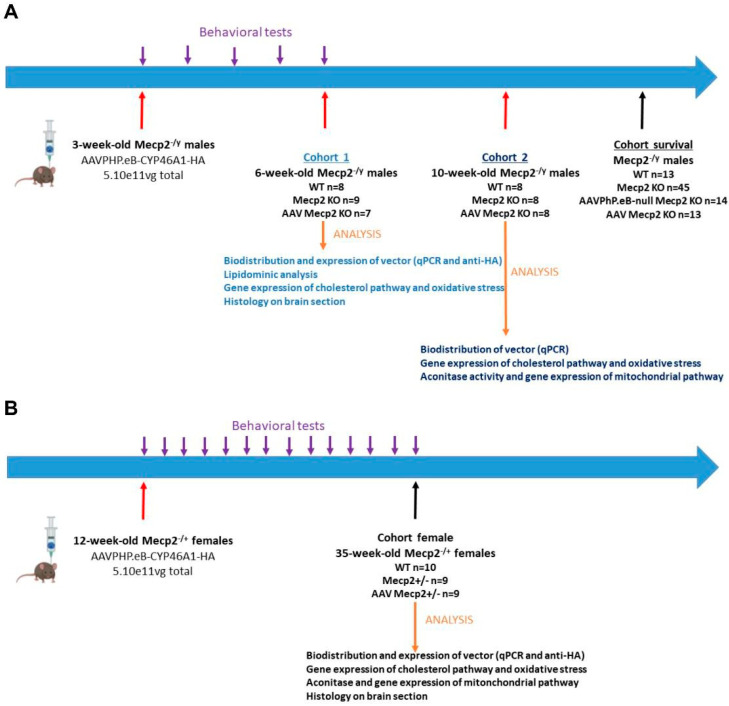
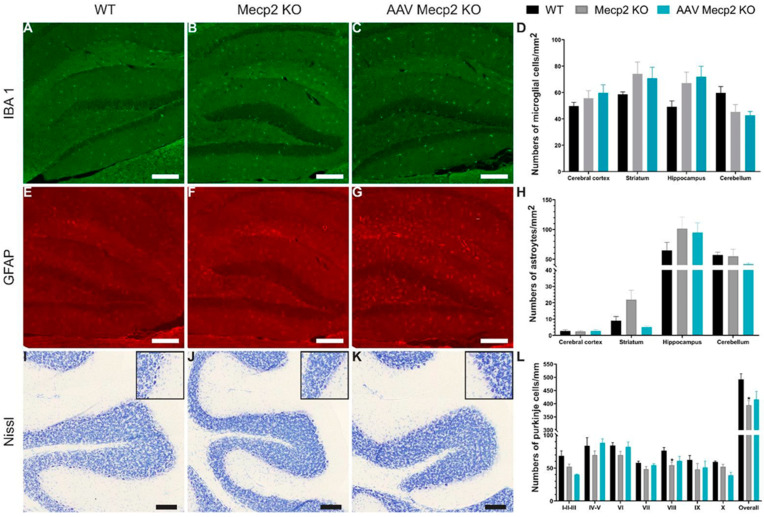
Rett syndrome (RTT) is a rare neurodevelopmental disorder caused by mutation in the X-linked gene methyl-CpG-binding protein 2 (Mecp2), a ubiquitously expressed transcriptional regulator. RTT results in mental retardation and developmental regression that affects approximately 1 in 10,000 females. Currently, there is no curative treatment for RTT. Thus, it is crucial to develop new therapeutic approaches for children suffering from RTT. Several studies suggested that RTT is linked with defects in cholesterol homeostasis, but for the first time, therapeutic evaluation is carried out by modulating this pathway. Moreover, AAV-based CYP46A1 overexpression, the enzyme involved in cholesterol pathway, has been demonstrated to be efficient in several neurodegenerative diseases. Based on these data, we strongly believe that CYP46A1 could be a relevant therapeutic target for RTT. Herein, we evaluated the effects of intravenous AAVPHP.eB-hCYP46A1-HA delivery in male and female Mecp2-deficient mice. The applied AAVPHP.eB-hCYP46A1 transduced essential neurons of the central nervous system (CNS). CYP46A1 overexpression alleviates behavioral alterations in both male and female Mecp2 knockout mice and extends the lifespan in Mecp2-deficient males. Several parameters related to cholesterol pathway are improved and correction of mitochondrial activity is demonstrated in treated mice, which highlighted the clear therapeutic benefit of CYP46A1 through the neuroprotection effect. IV delivery of AAVPHP.eB-CYP46A1 is perfectly well tolerated with no inflammation observed in the CNS of the treated mice. Altogether, our results strongly suggest that CYP46A1 is a relevant target and overexpression could alleviate the phenotype of Rett patients.
Keywords: AAVPHP.eB; Rett syndrome; cholesterol pathway; gene therapy.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures






Similar articles
-
Exploring the possible link between MeCP2 and oxidative stress in Rett syndrome.Free Radic Biol Med. 2015 Nov;88(Pt A):81-90. doi: 10.1016/j.freeradbiomed.2015.04.019. Epub 2015 May 8. Free Radic Biol Med. 2015. PMID: 25960047 Review.
-
RNA sequencing and proteomics approaches reveal novel deficits in the cortex of Mecp2-deficient mice, a model for Rett syndrome.Mol Autism. 2017 Oct 24;8:56. doi: 10.1186/s13229-017-0174-4. eCollection 2017. Mol Autism. 2017. PMID: 29090078 Free PMC article.
-
MECP2 mutations and clinical correlations in Greek children with Rett syndrome and associated neurodevelopmental disorders.Brain Dev. 2012 Jun;34(6):487-95. doi: 10.1016/j.braindev.2011.09.002. Epub 2011 Oct 6. Brain Dev. 2012. PMID: 21982064
-
CREB Signaling Is Involved in Rett Syndrome Pathogenesis.J Neurosci. 2017 Mar 29;37(13):3671-3685. doi: 10.1523/JNEUROSCI.3735-16.2017. Epub 2017 Mar 7. J Neurosci. 2017. PMID: 28270572 Free PMC article.
-
Rett syndrome: methyl-CpG-binding protein 2 mutations and phenotype-genotype correlations.Am J Med Genet. 2000 Summer;97(2):147-52. doi: 10.1002/1096-8628(200022)97:2<147::aid-ajmg6>3.0.co;2-o. Am J Med Genet. 2000. PMID: 11180222 Review.
References
-
- Weaving L.S., Christodoulou J., Williamson S.L., Friend K.L., McKenzie O.L.D., Archer H., Evans J., Clarke A., Pelka G.J., Tam P.P.L., et al. Mutations of CDKL5 Cause a Severe Neurodevelopmental Disorder with Infantile Spasms and Mental Retardation. Am. J. Hum. Genet. 2004;75:1079–1093. doi: 10.1086/426462. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
