

Hospital readmission following acute illness among children 2-23 months old in sub-Saharan Africa and South Asia: a secondary analysis of CHAIN cohort
- PMID: 38933099
- PMCID: PMC11200276
- DOI: 10.1016/j.eclinm.2024.102676
Hospital readmission following acute illness among children 2-23 months old in sub-Saharan Africa and South Asia: a secondary analysis of CHAIN cohort
Abstract
Background: Children in low and middle-income countries remain vulnerable following hospital-discharge. We estimated the incidence and correlates of hospital readmission among young children admitted to nine hospitals in sub-Saharan Africa and South Asia.
Methods: This was a secondary analysis of the CHAIN Network prospective cohort enrolled between 20th November 2016 and 31st January 2019. Children aged 2-23 months were eligible for enrolment, if admitted for an acute illness to one of the study hospitals. Exclusions were requiring immediate resuscitation, inability to tolerate oral feeds in their normal state of health, had suspected terminal illness, suspected chromosomal abnormality, trauma, admission for surgery, or their parent/caregiver was unwilling to participate and attend follow-up visits. Data from children discharged alive from the index admission were analysed for hospital readmission within 180-days from discharge. We examined ratios of readmission to post-discharge mortality rates. Using models with death as the competing event, we evaluated demographic, nutritional, clinical, and socioeconomic associations with readmission.
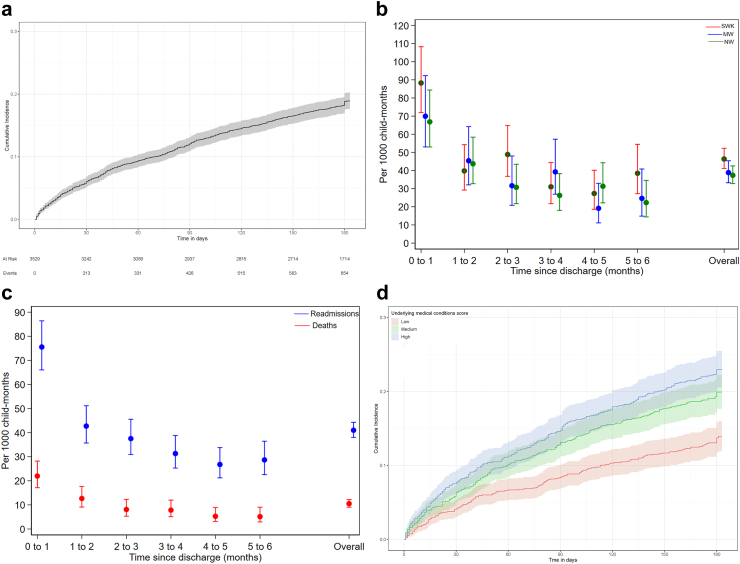
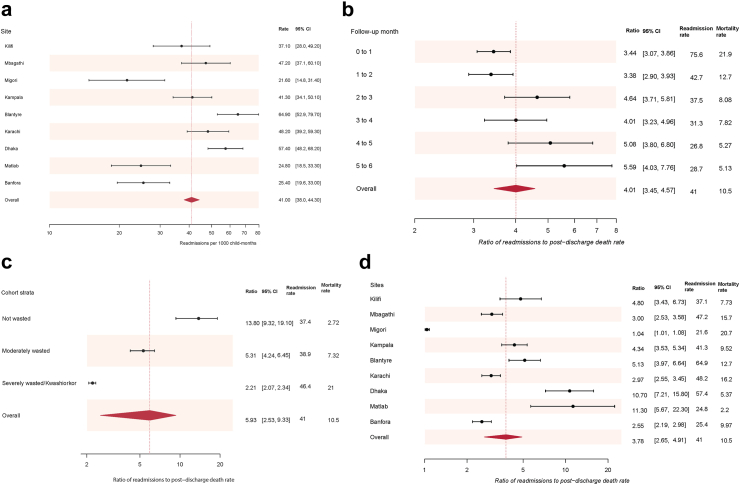
Findings: Of 2874 children (1239 (43%) girls, median (IQR) age 10.8 (6.8-15.6) months), 655 readmission episodes occurred among 506 (18%) children (198 (39%) girls): 391 (14%) with one, and 115 (4%) with multiple readmissions, with a rate of: 41.0 (95% CI 38.0-44.3) readmissions/1000 child-months. Median time to readmission was 42 (IQR 15-93) days. 460/655 (70%) and 195/655 (30%) readmissions occurred at index study hospital and non-study hospitals respectively. One-third (N = 213/655, 33%) of readmissions occurred within 30 days of index discharge. Sites with fewest readmissions had the highest post-discharge mortality. Most readmissions to study hospitals (371/450, 81%) were for the same illness as the index admission. Age, prior hospitalisation, chronic conditions, illness severity, and maternal mental health score, but not sex, nutritional status, or physical access to healthcare, were associated with readmission.
Interpretation: Readmissions may be appropriate and necessary to reduce post-discharge mortality in high mortality settings. Social and financial support, training on recognition of serious illness for caregivers, and improving discharge procedures, continuity of care and facilitation of readmission need to be tested in intervention studies. We propose the ratio of readmission to post-discharge mortality rates as a marker of overall post-discharge access and care.
Funding: The Bill & Melinda Gates Foundation (OPP1131320).
Keywords: Acute illness; Children; Low- and middle income; Post-discharge; Vulnerability.
© 2024 The Author(s).
Conflict of interest statement
Contributors received grant funding to their institutions from the Bill & Melinda Gates Foundation in relation to this study and allied work and declare no other competing interests.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
