Unveiling the enigma of acute kidney disease: predicting prognosis, exploring interventions, and embracing a multidisciplinary approach
- PMID: 38934037
- PMCID: PMC11237330
- DOI: 10.23876/j.krcp.23.289
Unveiling the enigma of acute kidney disease: predicting prognosis, exploring interventions, and embracing a multidisciplinary approach
Abstract
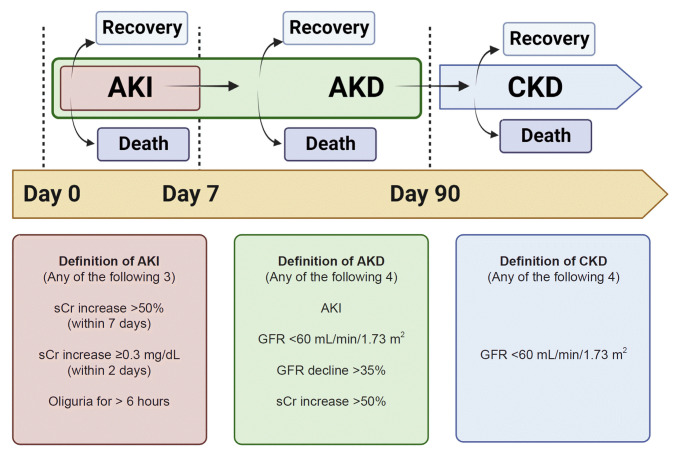
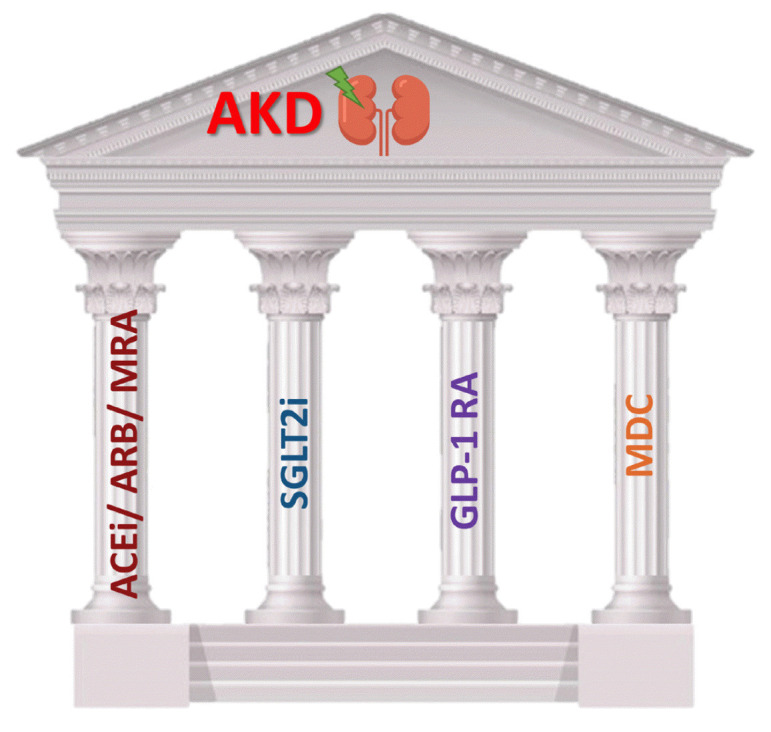
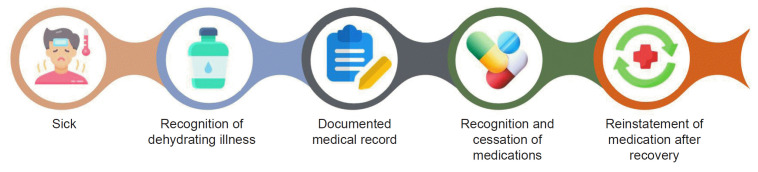
Acute kidney disease (AKD) is a critical transitional period between acute kidney injury and chronic kidney disease. The incidence of AKD following acute kidney injury is approximately 33.6%, and it can occur without identifiable preceding acute kidney injury. The development of AKD is associated with increased risks of chronic kidney disease, dialysis, and mortality. Biomarkers and subphenotypes are promising tools to predict prognosis in AKD. The complex clinical situations in patients with AKD necessitate a comprehensive and structured approach, termed "KAMPS" (kidney function check, advocacy, medications, pressure, sick day protocols). We introduce "MAND-MASS," an acronym devised to summarize the reconciliation of medications during episodes of acute illness, as a critical component of the sick day protocols at AKD. A multidisciplinary team care, consisting of nephrologists, pharmacists, dietitians, health educators, and nurses, is an optimal model to achieve the care bundle in KAMPS. Although the evidence for patients with AKD is still lacking, several potential pharmacological agents may improve outcomes, including but not limited to angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, mineralocorticoid receptor antagonists, sodium-glucose cotransporter 2 inhibitors, and glucagon-like peptide 1 receptor agonists. In conclusion, accurate prognosis prediction and effective treatment for AKD are critical yet unmet clinical needs. Future studies are urgently needed to improve patient care in this complex and rapidly evolving field.
Keywords: Acute kidney injury; Drug therapy; Patient care team; Prognosis.
Conflict of interest statement
Szu-Yu Pan was supported by the Ministry of Science and Technology, Taiwan (MOST, 111-2314-B-002-MY2). All other authors have no conflicts of interest to declare.
Figures
References
-
- Kellum JA, Lameire N, Aspelin P, et al. Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO clinical practice guideline for acute kidney injury. Kidney Int Suppl. 2012;2:1–138.
-
- Lameire NH, Levin A, Kellum JA, et al. Harmonizing acute and chronic kidney disease definition and classification: report of a Kidney Disease: Improving Global Outcomes (KDIGO) Consensus Conference. Kidney Int. 2021;100:516–526. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous