

Revised criteria for diagnosis and staging of Alzheimer's disease: Alzheimer's Association Workgroup
- PMID: 38934362
- PMCID: PMC11350039
- DOI: 10.1002/alz.13859
Revised criteria for diagnosis and staging of Alzheimer's disease: Alzheimer's Association Workgroup
Abstract
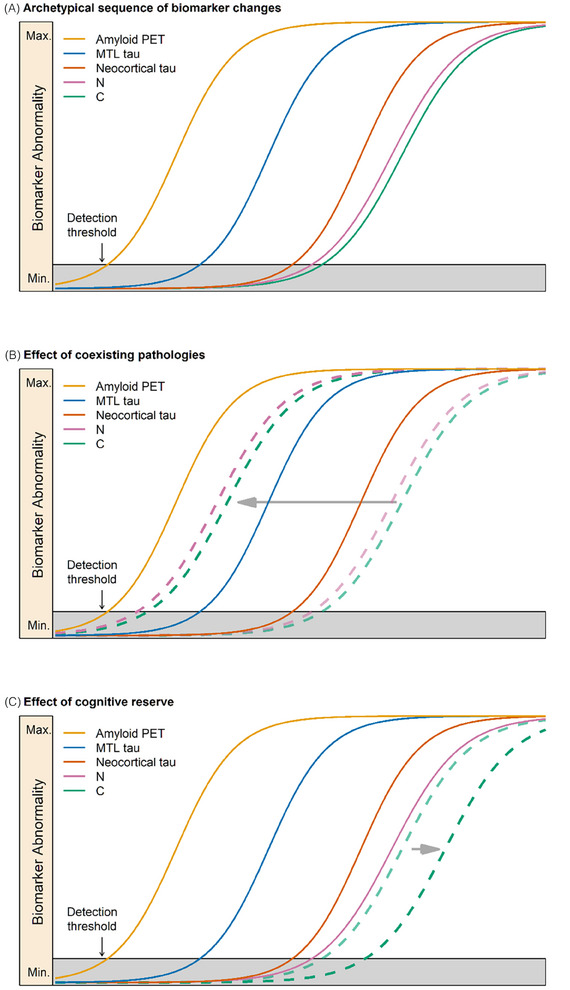
The National Institute on Aging and the Alzheimer's Association convened three separate work groups in 2011 and single work groups in 2012 and 2018 to create recommendations for the diagnosis and characterization of Alzheimer's disease (AD). The present document updates the 2018 research framework in response to several recent developments. Defining diseases biologically, rather than based on syndromic presentation, has long been standard in many areas of medicine (e.g., oncology), and is becoming a unifying concept common to all neurodegenerative diseases, not just AD. The present document is consistent with this principle. Our intent is to present objective criteria for diagnosis and staging AD, incorporating recent advances in biomarkers, to serve as a bridge between research and clinical care. These criteria are not intended to provide step-by-step clinical practice guidelines for clinical workflow or specific treatment protocols, but rather serve as general principles to inform diagnosis and staging of AD that reflect current science. HIGHLIGHTS: We define Alzheimer's disease (AD) to be a biological process that begins with the appearance of AD neuropathologic change (ADNPC) while people are asymptomatic. Progression of the neuropathologic burden leads to the later appearance and progression of clinical symptoms. Early-changing Core 1 biomarkers (amyloid positron emission tomography [PET], approved cerebrospinal fluid biomarkers, and accurate plasma biomarkers [especially phosphorylated tau 217]) map onto either the amyloid beta or AD tauopathy pathway; however, these reflect the presence of ADNPC more generally (i.e., both neuritic plaques and tangles). An abnormal Core 1 biomarker result is sufficient to establish a diagnosis of AD and to inform clinical decision making throughout the disease continuum. Later-changing Core 2 biomarkers (biofluid and tau PET) can provide prognostic information, and when abnormal, will increase confidence that AD is contributing to symptoms. An integrated biological and clinical staging scheme is described that accommodates the fact that common copathologies, cognitive reserve, and resistance may modify relationships between clinical and biological AD stages.
Keywords: Alzheimer's disease diagnosis; Alzheimer's disease imaging; Alzheimer's disease staging; amyloid positron emission tomography; biofluid biomarkers Alzheimer's disease; biomarkers Alzheimer's disease; preclinical Alzheimer's disease; tau positron emission tomography.
© 2024 The Authors. Alzheimer's & Dementia published by Wiley Periodicals LLC on behalf of Alzheimer's Association.
Conflict of interest statement
Clifford R. Jack Jr. is employed by Mayo Clinic. Within the past 36 months, he served on a Data Safety Monitoring Board for Roche pro bono; no payments to the individual or institution were involved. In addition, he holds index funds. J. Scott Andrews is employed by Takeda Pharmaceuticals and is a minor shareholder for the company. He has a leadership or fiduciary role in the Clinical Trials on Alzheimer's Disease (CTAD) Task Force—Clinical Meaningfulness and Optimizing Therapies, AD PACE Executive Steering Committee, and UsAgainstAlzheimer's—Clinical Meaningfulness Forum. He is a former employee of Eli Lilly and Company and is a minor shareholder for the company. Thomas G. Beach is employed by Banner Health. He has received consulting fees from Aprinoia Therapeutics and Acadia Pharmaceuticals. He consulted for Biogen. He has received payment or honoraria from the World PD Coalition, Mayo Clinic Florida, Stanford University, and the IOS Press‐Journal of Parkinson's Disease and support for attending meetings from the Alzheimer's Association, AD/PD/Kenes Group, Mayo Clinic Florida, Universitätsklinikum Hamburg‐Eppendorf, and the International Movement Disorders Association. In addition he has recieved funds from the National Institutes of Health for reviewing grant proposals. He also has a leadership/fiduciary role and stock options with Vivid Genomics. Teresa Burracchio is employed by the US Food and Drug Administration and has no financial conflicts to disclose. Billy Dunn is a consultant and has received consulting fees for his role as an advisor for Arch Venture Partners, Cerveau Technologies, Epilepsy Foundation, F‐PRIME Capital, Loulou Foundation, and Michael J. Fox Foundation. He has held a past position of leadership or fiduciary role in the Virginia Neurological Society (past president) and Prothena Inc. (Director). He holds stock options with Prothena Inc. Ana Graf is employed by Novartis Pharma AG and has stock options in the company. Oskar Hansson is employed by Lund University. He has grants or contracts from ADx, AVID Radiopharmaceuticals, Biogen, Eli Lilly, Eisai, Fujirebio, GE Healthcare, Pfizer, and Roche. He also has been paid consulting fees by AC Immune, Amylyx, Alzpath, BioArctic, Biogen, Cerveau, Eisai, Eli Lilly, Fujirebio, Genentech, Merck, Novartis, Novo Nordisk, Roche, Sanofi, and Siemens. In the past 2 years, he has received consultancy/speaker fees from AC Immune, Alzpath, BioArctic, Biogen, Bristol Meyer Squibb, Cerveau, Eisai, Eli Lilly, Fujirebio, Merck, Novartis, Novo Nordisk, Roche, Sanofi, and Siemens. Carole Ho is employed by Denali Therapeutics. She has stock options with Denali Therapeutics. She is also a Board Director for Beam Therapeutics and NGM Therapeutics and has stock options with both companies. William Jagust is employed by University of California, Berkley. He has received consulting fees from Biogen, Clario, Eisai, Lilly, and Prothena and has stock with Optoceutics and Molecular Medicine. Eric McDade is employed by Washington University, St Louis. He has received royalties for work on “Methods of diagnosing AD with phosphorylation changes,” which is licensed to C2N with royalties to himself and Washington University. He has received consulting fees from Alzamend (SAB member), Sanofi, AstraZeneca, Roche, Grifols, Merck, and Sage. He has also received payments from Neurology Live; Kaplan‐Projects in Knowledge; and support for travel from Foundation Alzheimer, Alzheimer's Association, and Eisai. He has a patent planned, issued, or pending on “Methods of diagnosing AD with phosphorylation changes” and has participated on a Data Safety Monitoring Board or Advisory Board for Alector and Eli Lilly, both roles for which he was paid. He has a leadership/fiduciary role in Alzamend (paid). Jose Luis Molinuevo is a full‐time employee of H. Lundbeck A/S. Ozioma Okonkwo is employed by University of Wisconsin School of Medicine & Public Health. He has received consulting fees from Mayo Clinic Rochester and IUPUI, and has held a leadership or fiduciary role in the International Neuropsychological Society (Board Member) and previously held an advisory role for Society for Black Neuropsychology. Luca Pani is employed by the University of Miami and the University of Modena and Reggio Emilia and has no financial conflicts to disclose. In unrelated areas, he holds options/stocks from Relmada Therapeutics (US) and NetraMark (Canada). Michael Rafii is employed by University of Southern California and the Alzheimer's Therapeutics Research Institute (ATRI). He has received consulting fees from AC Immune and Ionis. He has participated on a Data Safety Monitoring Board or Advisory Board for Alzheon, Aptah Bio, Biohaven, Embic, Keystone Bio, Prescient Imaging, and Positrigo. Philip Scheltens is employed by Life Science Partners and is Professor Emeritus Amsterdam University Medical Center. He has an unpaid leadership position as Chair of World Dementia Council. He holds stock options in EQT AB. Eric Siemers is employed by Acumen Pharmaceuticals, Inc. He has received consulting fees from Cogstate Ltd., Cortexyme Inc., Partner Therapeutics Inc., Vaccinex Inc., Gates Ventures LLC, and Hoffman La Roche Ltd and payments were made to Siemers Integration LLC. He has participated on a Data Safety Monitoring Board for Hoffman La Roche Ltd. and has had a leadership or fiduciary role with the Alzheimer's Association and BrightFocus Foundation, both unpaid. He holds stock options and is a shareholder for Acumen Pharmaceuticals, and is a shareholder for Eli Lilly and Company. Heather Snyder is a full‐time employee of the Alzheimer's Association, Chicago, IL, and has a spouse who is employed by Abbott Laboratories in an unrelated area. She has no financial conflicts to disclose. Reisa Sperling is employed by Brigham and Women's Hospital. She has received consulting fees from Abbvie, AC Immune, Acumen, Alector, Alnylam, Biohaven, Bristol‐Myers Squibb, Cytox, Genentech, Ionis, Janssen, Merck, NervGen, Neuraly, Neurocentria, Oligomerix, Prothena, Roche, Shionogi, and Vaxxinity. Charlotte E. Teunissen is employed by Amsterdam UMC. She is recipient of ABOARD, which is a public–private partnership receiving funding from ZonMW (#73305095007) and Health∼Holland, Topsector Life Sciences & Health (PPP‐allowance; #LSHM20106). She is also a contract researcher for ADx Neurosciences, AC‐Immune, Aribio, Axon Neurosciences, Beckman‐Coulter, BioConnect, Bioorchestra, Brainstorm Therapeutics, Celgene, Cognition Therapeutics, EIP Pharma, Eisai, Eli Lilly, Fujirebio, Grifols, Instant Nano Biosensors, Merck, Novo Nordisk, Olink, PeopleBio, Quanterix, Roche, Siemens, Toyama, Vivoryon, and the European Commission. She has received payment or honoraria from Eli Lilly, Grifols, Novo Nordisk, Olink, and Roche, where all payments were made to her institution. She also serves on editorial boards of Medidact Neurologie/Springer; and on
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
- Eli Lilly
- Eisai
- RF1 AG052324/AG/NIA NIH HHS/United States
- R01AG062167/Hoffmann-La Roche
- Alzheimer Netherlands
- R01 AG066203/AG/NIA NIH HHS/United States
- R01 AG070028/AG/NIA NIH HHS/United States
- Toyama
- Health Holland
- U19 AG073153/AG/NIA NIH HHS/United States
- AVID Radiopharmaceuticals
- Avid Radiopharmaceuticals/Eli Lilly
- Novo Nordisk
- Biogen
- Alexander family professorship
- 860197/Research of the European Commission
- R01 AG077507/AG/NIA NIH HHS/United States
- 101034344/Innovative Medicines Initiatives 3TR
- BrightFocus Foundation
- The Selfridges Group Foundation
- Michael J. Fox Foundation for Parkinson's Research
- ALZ/Alzheimer's Association/United States
- U19AG078109/Hoffmann-La Roche
- R01 AG062167/AG/NIA NIH HHS/United States
- 831434/Innovative Medicines Initiatives 3TR
- U19AG024904/Hoffmann-La Roche
- C2N Diagnostics
- R01 AG027161/AG/NIA NIH HHS/United States
- R01AG077507/Hoffmann-La Roche
- GHR Foundation
- U19 AG024904/AG/NIA NIH HHS/United States
- Gates Foundation
- GE Healthcare
- NWO_/Dutch Research Council/Netherlands
- Alzheon
- NH/NIH HHS/United States
- Alzheimer Drug Discovery Foundation
- State of Arizona
- U19 AG078109/AG/NIA NIH HHS/United States
- R01AG070028/Hoffmann-La Roche
- Roche/Genentech
- 10510032120003/TAP-dementia
- RF1AG052324/Hoffmann-La Roche
- AC Immune
- Fujirebio
- National MS Society
- U19AG073153/Hoffmann-La Roche
- Veterans Administration
LinkOut - more resources
Full Text Sources
Medical
