

Safety and Immunogenicity of mRNA-1010, an Investigational Seasonal Influenza Vaccine, in Healthy Adults: Final Results From a Phase 1/2 Randomized Trial
- PMID: 38934845
- PMCID: PMC11793046
- DOI: 10.1093/infdis/jiae329
Safety and Immunogenicity of mRNA-1010, an Investigational Seasonal Influenza Vaccine, in Healthy Adults: Final Results From a Phase 1/2 Randomized Trial
Abstract
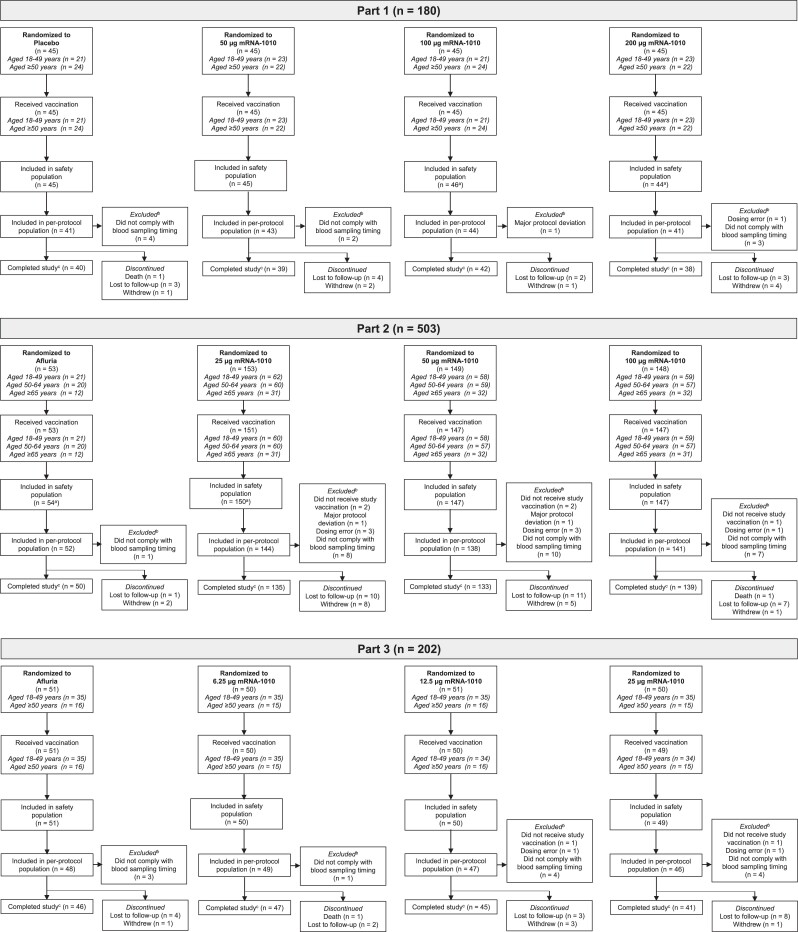
Background: Seasonal influenza remains a global public health concern. A messenger RNA (mRNA)-based quadrivalent seasonal influenza vaccine, mRNA-1010, was investigated in a first-in-human, phase 1/2 clinical trial conducted in 3 parts.
Methods: In parts 1 to 3 of this stratified observer-blind study, adults aged ≥18 years were randomly assigned to receive a single dose (6.25-200 µg) of mRNA-1010 or placebo (part 1) or an active comparator (Afluria; parts 2 and 3). Primary study objectives were assessment of safety, reactogenicity, and humoral immunogenicity of mRNA-1010, placebo (part 1), or active comparator (parts 2 and 3). Exploratory end points included assessment of cellular immunogenicity (part 1) and antigenic breadth against vaccine heterologous strains (A/H3N2; parts 1 and 2).
Results: In all study parts, solicited adverse reactions were reported more frequently for mRNA-1010 than placebo or Afluria, and most were grade 1 or 2 in severity. No vaccine-related serious adverse events or deaths were reported. In parts 1 and 2, a single dose of mRNA-1010 (25-200 µg) elicited robust day 29 hemagglutination inhibition titers that persisted through 6 months. In part 3, lower doses of mRNA-1010 (6.25-25 µg) elicited day 29 hemagglutination inhibition titers that were higher or comparable to those of Afluria for influenza A strains. When compared with Afluria, mRNA-1010 (50 µg) elicited broader A/H3N2 antibody responses (part 2). mRNA-1010 induced greater T-cell responses than placebo at day 8 that were sustained or stronger at day 29 (part 1).
Conclusions: Data support the continued development of mRNA-1010 as a seasonal influenza vaccine.
Clinical trials registration: NCT04956575 (https://clinicaltrials.gov/study/NCT04956575).
Keywords: influenza; messenger RNA; phase 1/2; randomized clinical trial; vaccine.
© The Author(s) 2024. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. J. A., I. T. L., L. C., K. S., A. A., D. S., A. C., A. P., S. M., H.-H. K., C. H., R. C., W. H., R. N., and R. P. are employees of and shareholders in Moderna, Inc. D. E. has no reported conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures




References
-
- World Health Organization . Vaccines against influenza: WHO position paper—May 2022. Wkly Epidemiol Rec 2022; 97:185–208.
-
- Centers for Disease Control and Prevention . Vaccine effectiveness: how well do flu vaccines work? https://www.cdc.gov/flu/vaccines-work/vaccineeffect.htm. Accessed 21 June 2022.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
