

Clinical Implementation of DIGEST as an Evidence-Based Practice Tool for Videofluoroscopy in Oncology: A Six-Year Single Institution Implementation Evaluation
- PMID: 38935170
- PMCID: PMC11792177
- DOI: 10.1007/s00455-024-10721-2
Clinical Implementation of DIGEST as an Evidence-Based Practice Tool for Videofluoroscopy in Oncology: A Six-Year Single Institution Implementation Evaluation
Abstract
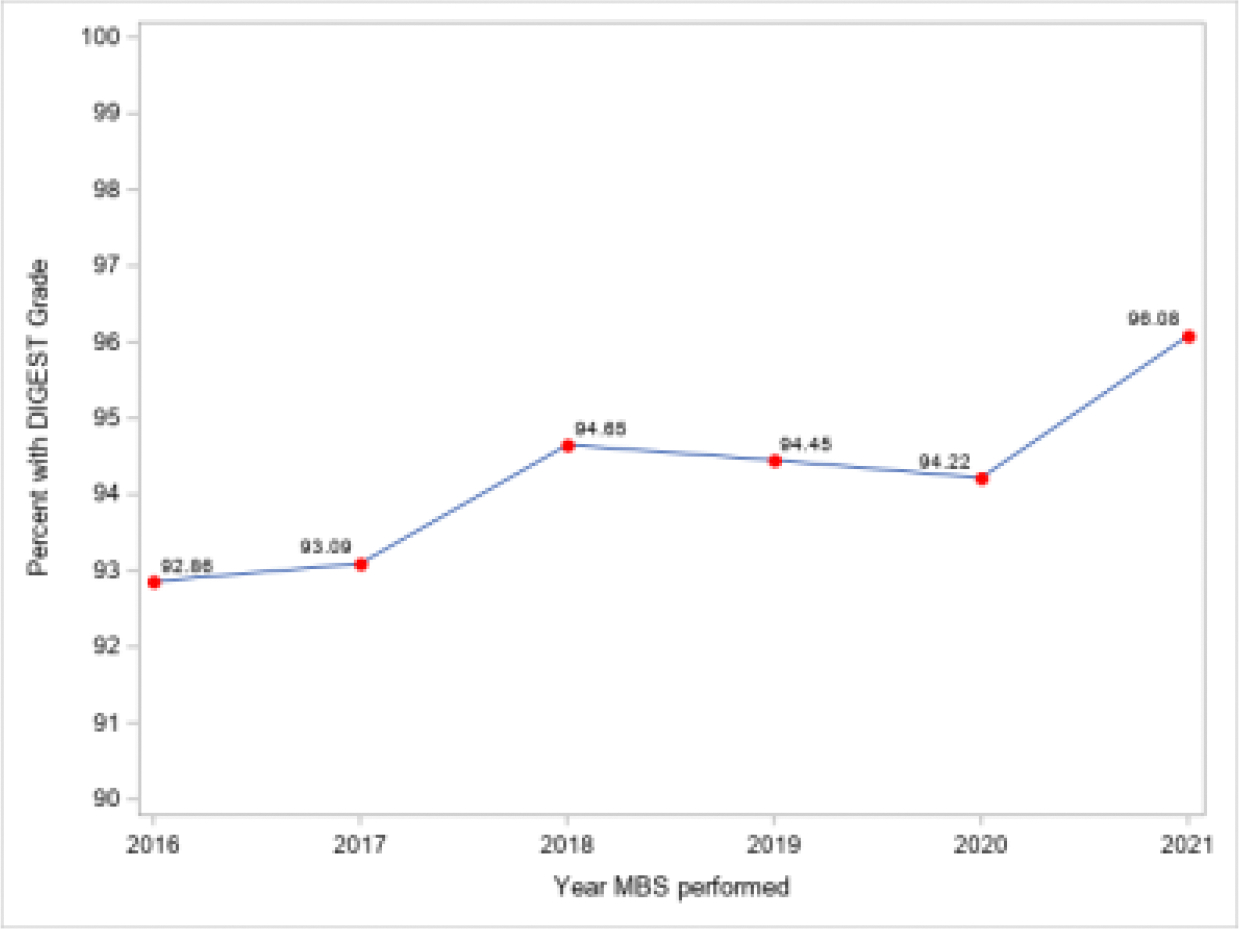
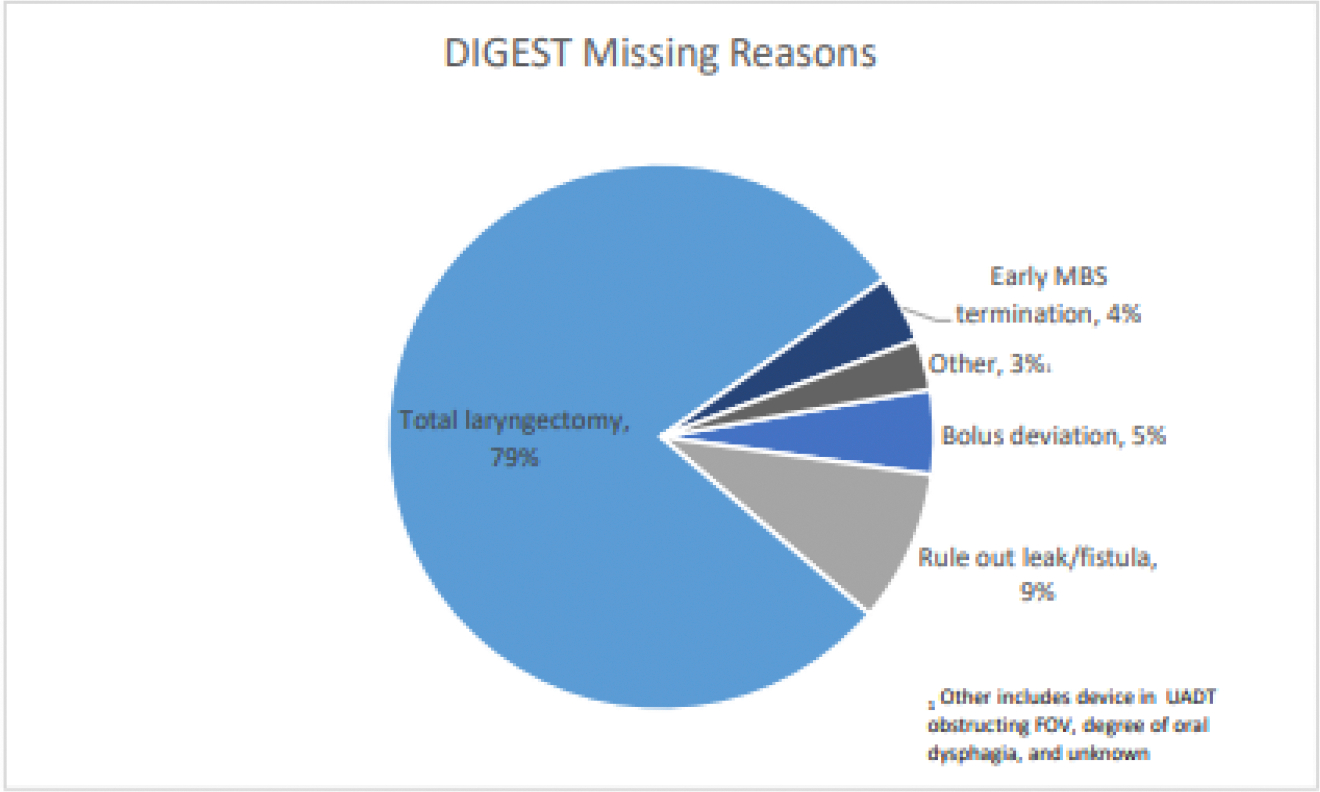
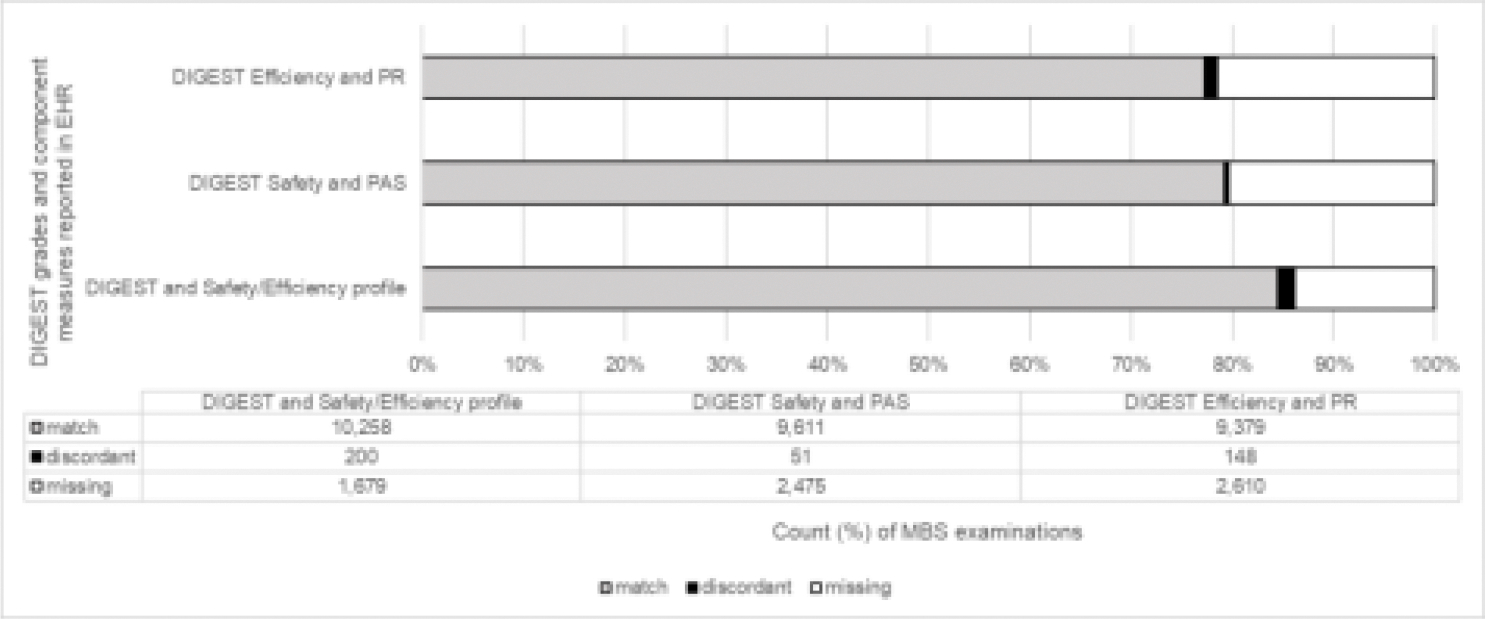
Clinical implementation of evidence-based practice (EBP) tools is a healthcare priority. The Dynamic Grade of Swallowing Toxicity (DIGEST) is an EBP tool developed in 2016 for videofluoroscopy in head and neck (H&N) oncology with clinical implementation as a goal. We sought to examine: (1) feasibility of clinical implementation of DIGEST in a national comprehensive cancer center, and (2) fidelity of DIGEST adoption in real-world practice. A retrospective implementation evaluation was conducted in accordance with the STARI framework. Electronic health record (EHR) databases were queried for all consecutive modified barium swallow (MBS) studies conducted at MD Anderson Cancer Center from 2016 to 2021. Implementation outcomes included: feasibility as measured by DIGEST reporting in EHR (as a marker of clinical use) and fidelity as measured by accuracy of DIGEST reporting relative to the decision-tree logic (penetration-aspiration scale [PAS], residue, and Safety [S] and Efficiency [E] grades). Contextual factors examined included year, setting, cancer type, MBS indication, and provider. 13,055 MBS were conducted by 29 providers in 7,842 unique patients across the lifespan in diverse oncology populations (69% M; age 1-96 years; 58% H&N cancer; 10% inpatient, 90% outpatient). DIGEST was reported in 12,137/13,088 exams over the 6-year implementation period representing 93% (95% CI: 93-94%) adoption in all exams and 99% (95% CI: 98-99%) of exams excluding the total laryngectomy population (n = 730). DIGEST reporting varied modestly by year, cancer type, and setting/provider (> 91% in all subgroups, p < 0.001). Accuracy of DIGEST reporting was high for overall DIGEST (incorrect SE profile 1.6%, 200/12,137), DIGEST-safety (incorrect PAS 0.4% 51/12,137) and DIGEST-efficiency (incorrect residue 1.2%, 148/12,137). Clinical implementation of DIGEST was feasible with high fidelity in a busy oncology practice across a large number of providers. Adoption of the tool across the lifespan in diverse cancer diagnoses may motivate validation beyond H&N oncology.
Keywords: DIGEST; Evidence-based practice; Implementation science; Modified barium swallow; Videofluoroscopy.
© 2024. The Author(s), under exclusive licence to Springer Science+Business Media, LLC, part of Springer Nature.
Conflict of interest statement
Declarations. Disclosure: Research reported in this publication was partially supported by the National Institutes of Health (NIH), National Cancer Institute (NCI) under award R01CA271223. The Cancer Center Support Grant (NCI Grant P30 CA016672) provided partial support of this work. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Figures

Similar articles
-
Compensatory Swallowing Strategies Recommended in Oncology Practice: Practice Patterns and Relationship to Dynamic Imaging Grade of Swallowing Toxicity (DIGEST) Grades.Dysphagia. 2025 Aug;40(4):998-1007. doi: 10.1007/s00455-024-10799-8. Epub 2025 Jan 18. Dysphagia. 2025. PMID: 39827333
-
Fluoroscopy Time of Radiologist-Monitored Modified Barium Swallow Exams in Oncology: A 3-year Single Institution Retrospective Study.Dysphagia. 2025 Mar 29. doi: 10.1007/s00455-025-10822-6. Online ahead of print. Dysphagia. 2025. PMID: 40156643
-
Refining measurement of swallowing safety in the Dynamic Imaging Grade of Swallowing Toxicity (DIGEST) criteria: Validation of DIGEST version 2.Cancer. 2022 Apr 1;128(7):1458-1466. doi: 10.1002/cncr.34079. Epub 2022 Jan 5. Cancer. 2022. PMID: 34985765 Free PMC article.
-
Current practice in paediatric videofluoroscopy.Pediatr Radiol. 2006 Sep;36(9):911-9. doi: 10.1007/s00247-006-0124-3. Epub 2006 Mar 22. Pediatr Radiol. 2006. PMID: 16552584 Review.
-
The modified barium swallow and the functional endoscopic evaluation of swallowing.Otolaryngol Clin North Am. 2013 Dec;46(6):1009-22. doi: 10.1016/j.otc.2013.08.001. Epub 2013 Oct 8. Otolaryngol Clin North Am. 2013. PMID: 24262956 Review.
Cited by
-
Validation of the Dynamic Imaging Grade of Swallowing Toxicity for Amyotrophic Lateral Sclerosis.Neurogastroenterol Motil. 2025 Jun;37(6):e70008. doi: 10.1111/nmo.70008. Epub 2025 Mar 3. Neurogastroenterol Motil. 2025. PMID: 40033457 Free PMC article.
References
-
- Balas EA, Boren SA. Managing Clinical Knowledge for Health Care Improvement. Yearb Med Inform. 2000;(1):65–70. - PubMed
-
- Grant J, Green L, Mason B. Basic research and health: a reassessment of the scientific basis for the support of biomedical science. Research Evaluation. 2003;12(3):217–224. doi:10.3152/147154403781776618 - DOI
-
- Vallino-Napoli LD, Reilly S. Evidence-based health care: A survey of speech pathology practice. Advances in Speech Language Pathology. 2004/06/01 2004;6(2):107–112.vdoi:10.1080/14417040410001708530 - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
