

Impact of intensive prone position therapy on outcomes in intubated patients with ARDS related to COVID-19
- PMID: 38935175
- PMCID: PMC11211313
- DOI: 10.1186/s13613-024-01340-z
Impact of intensive prone position therapy on outcomes in intubated patients with ARDS related to COVID-19
Erratum in
-
Correction to: Impact of intensive prone position therapy on outcomes in intubated patients with ARDS related to COVID-19.Ann Intensive Care. 2024 Sep 11;14(1):142. doi: 10.1186/s13613-024-01374-3. Ann Intensive Care. 2024. PMID: 39259402 Free PMC article. No abstract available.
Abstract
Background: Previous retrospective research has shown that maintaining prone positioning (PP) for an average of 40 h is associated with an increase of survival rates in intubated patients with COVID-19-related acute respiratory distress syndrome (ARDS). This study aims to determine whether a cumulative PP duration of more than 32 h during the first 2 days of intensive care unit (ICU) admission is associated with increased survival compared to a cumulative PP duration of 32 h or less.
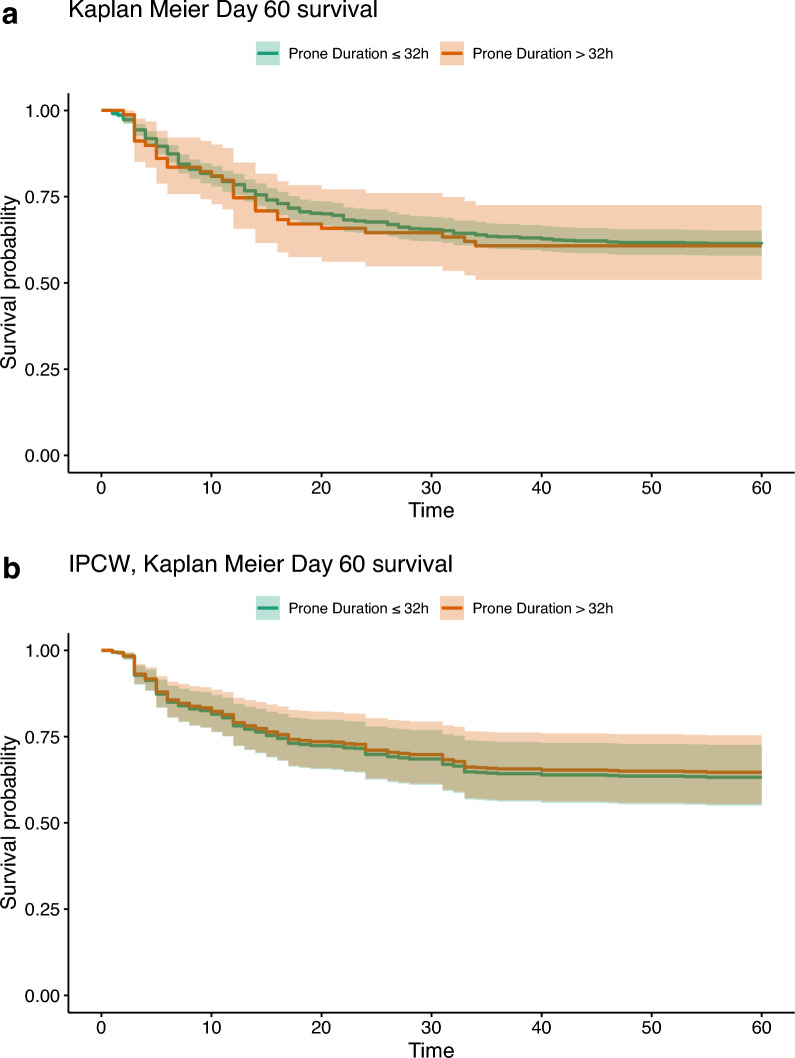
Methods: This study is an ancillary analysis from a previous large international observational study involving intubated patients placed in PP in the first 48 h of ICU admission in 149 ICUs across France, Belgium and Switzerland. Given that PP is recommended for a 16-h daily duration, intensive PP was defined as a cumulated duration of more than 32 h during the first 48 h, whereas standard PP was defined as a duration equal to or less than 32 h. Patients were followed-up for 90 days. The primary outcome was mortality at day 60. An Inverse Probability Censoring Weighting (IPCW) Cox model including a target emulation trial method was used to analyze the data.
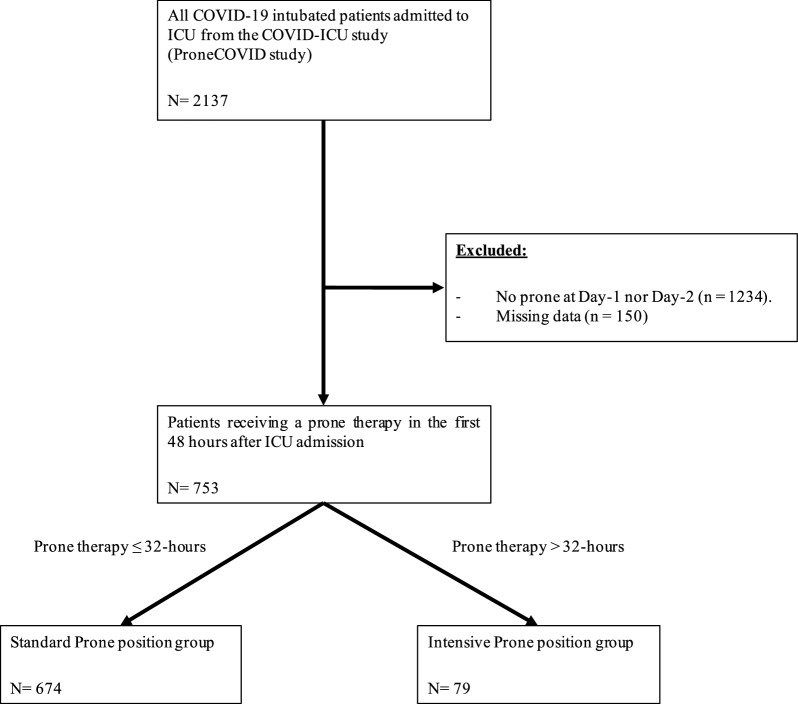
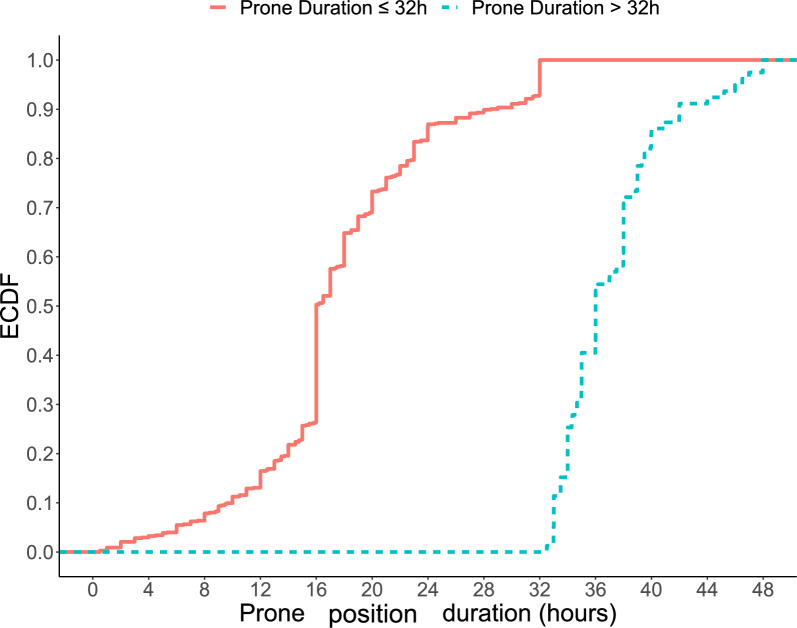
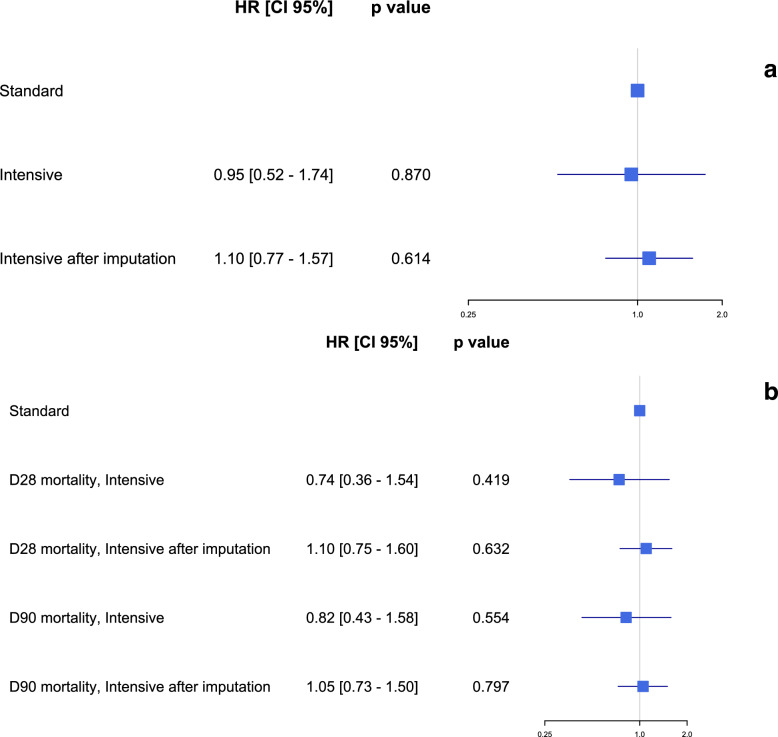
Results: Out of 2137 intubated patients, 753 were placed in PP during the first 48 h of ICU admission. The intensive PP group (n = 79) had a median PP duration of 36 h, while standard PP group (n = 674) had a median of 16 h during the first 48 h. Sixty-day mortality rate in the intensive PP group was 39.2% compared to 38.7% in the standard PP group (p = 0.93). Twenty-eight-day and 90-day mortality as well as the ventilator-free days until day 28 were similar in both groups. After IPCW, there was no significant difference in mortality at day 60 between the two-study groups (HR 0.95 [0.52-1.74], p = 0.87 and HR 1.1 [0.77-1.57], p = 0.61 in complete case analysis or in multiple imputation analysis, respectively).
Conclusions: This secondary analysis of a large multicenter European cohort of intubated patients with ARDS due to COVID-19 found that intensive PP during the first 48 h did not provide a survival benefit compared to standard PP.
Keywords: Acute respiratory distress syndrome; COVID-19; Intensive care unit; Intensive prone position; Intubation; Mortality.
© 2024. The Author(s).
Conflict of interest statement
All authors declare no conflicts of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous
