

Practical guidance for assessing and reporting lymphovascular space invasion (LVSI) in endometrial carcinoma
- PMID: 38937066
- PMCID: PMC11649510
- DOI: 10.1111/his.15272
Practical guidance for assessing and reporting lymphovascular space invasion (LVSI) in endometrial carcinoma
Abstract
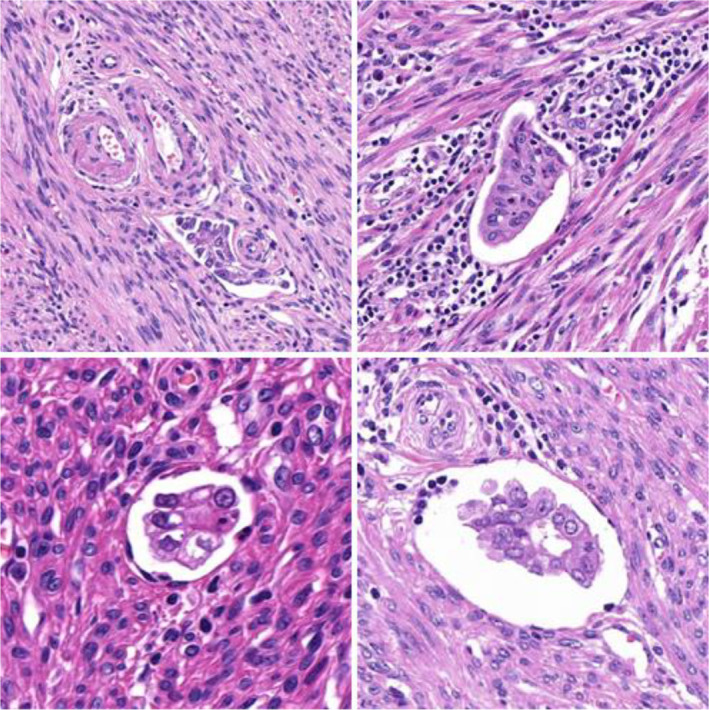
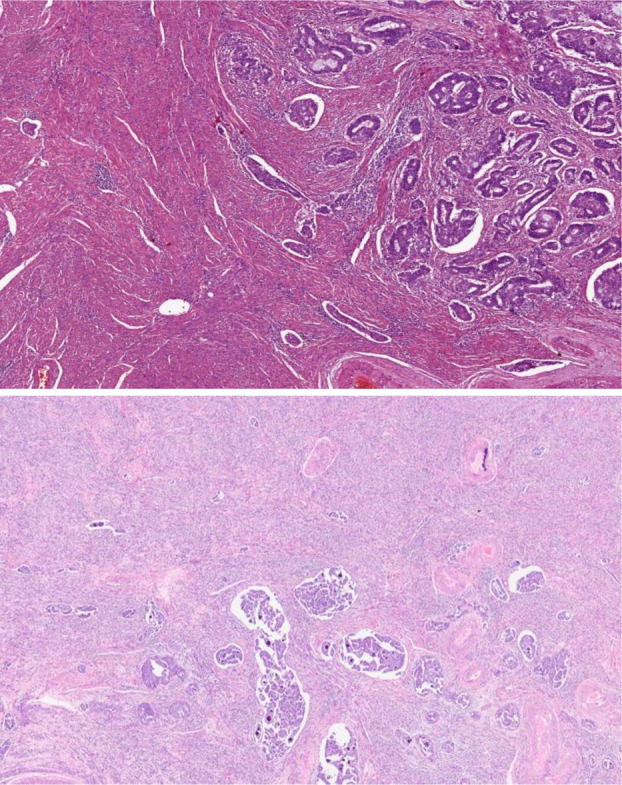
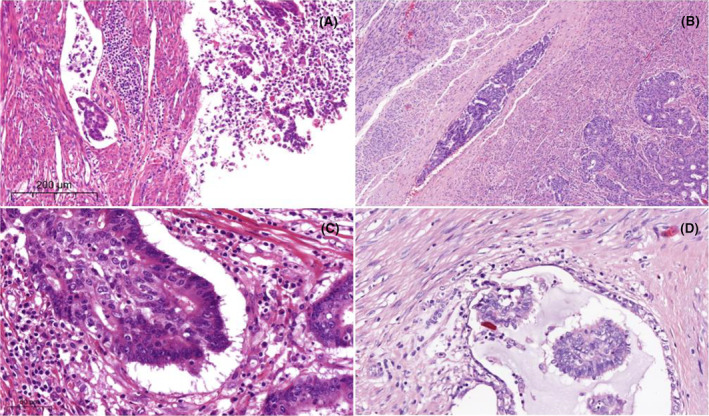
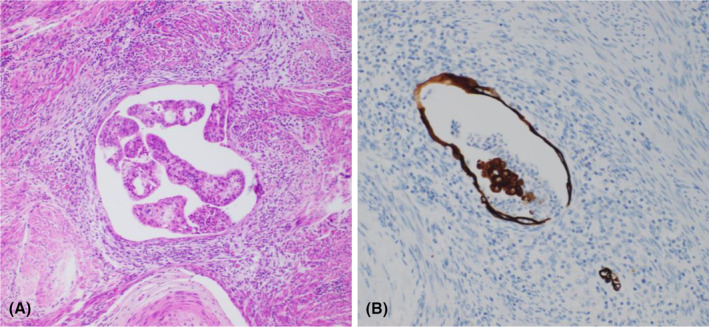
Lymphovascular space invasion (LVSI) is an important prognostic parameter in endometrial carcinoma (EC) and has gained increasing interest in recent years due to an expanding body of evidence of its independent prognostic value, especially when the presence of LVSI is quantified. A key strength of LVSI as a prognostic factor is that it can be detected on routine microscopic examination, without ancillary tests, and thus can be used in low-resource settings. A weakness, however, is the lack of uniformly applied criteria for assessment and quantification of LVSI, resulting in interobserver variation in diagnosis. This is confounded by artefacts and other morphological features that may mimic LVSI (commonly referred to as pseudo-LVSI). Despite these issues, multiple studies have shown that LVSI is strongly associated with lymph node (LN) metastasis and is an independent risk factor for LN recurrence and distant metastasis. Consequently, the presence of substantial/extensive LVSI has become an important consideration in formulating adjuvant treatment recommendations in patients with EC, and this has been incorporated in the recent International Federation of Gynecology and Obstetrics (FIGO) 2023 staging system. Herein, we review the current literature on LVSI in EC and discuss its role as a prognostic marker, the reproducibility of LVSI assessment and distinction between LVSI and its mimics. We provide illustrations of key diagnostic features and discuss the two-tiered (none/focal versus substantial) system of LVSI classification. This work is intended to provide guidance to practising pathologists and unify the approach towards LVSI assessment in EC.
Keywords: endometrial carcinoma; lymphovascular space invasion (LVSI); mimics; prognosis; reproducibility.
© 2024 The Author(s). Histopathology published by John Wiley & Sons Ltd.
Conflict of interest statement
No conflict of interest.
Figures
Similar articles
-
Is Substantial Lymphovascular Space Invasion Prognostic for Clinical Outcomes in Type II Endometrial Cancer?Clin Oncol (R Coll Radiol). 2022 Jul;34(7):452-458. doi: 10.1016/j.clon.2022.02.018. Epub 2022 Mar 6. Clin Oncol (R Coll Radiol). 2022. PMID: 35264314 Free PMC article.
-
Is the risk of substantial LVSI in stage I endometrial cancer similar to PORTEC in the North American population? - A single-institution study.Gynecol Oncol. 2020 Oct;159(1):23-29. doi: 10.1016/j.ygyno.2020.07.024. Epub 2020 Jul 25. Gynecol Oncol. 2020. PMID: 32718729
-
Reproducibility of lymphovascular space invasion (LVSI) assessment in endometrial cancer.Histopathology. 2019 Jul;75(1):128-136. doi: 10.1111/his.13871. Epub 2019 Jun 10. Histopathology. 2019. PMID: 31155736 Free PMC article. Clinical Trial.
-
Lymphovascular Space Invasion as a Risk Factor in Early Endometrial Cancer.Curr Oncol Rep. 2016 Apr;18(4):24. doi: 10.1007/s11912-016-0505-1. Curr Oncol Rep. 2016. PMID: 26922330 Review.
-
LVSI positive and NX in early endometrial cancer: Surgical restaging (and no further treatment if N0), or adjuvant ERT?Gynecol Oncol. 2020 Jan;156(1):243-250. doi: 10.1016/j.ygyno.2019.09.016. Epub 2019 Nov 5. Gynecol Oncol. 2020. PMID: 31703813 Review.
Cited by
-
The past, present, and future of FIGO staging of endometrial cancer.J Gynecol Oncol. 2025 Jul;36(4):e105. doi: 10.3802/jgo.2025.36.e105. Epub 2025 Apr 14. J Gynecol Oncol. 2025. PMID: 40350708 Free PMC article. Review.
References
-
- Matias‐Guiu X, Selinger CI, Anderson L et al. Data set for the reporting of endometrial cancer: recommendations from the international collaboration on cancer reporting (ICCR). Int. J. Gynecol. Pathol. 2022; 41; S90–S118. - PubMed
-
- Geels YP, Pijnenborg JM, van den Berg‐van Erp SH et al. Endometrioid endometrial carcinoma with atrophic endometrium and poor prognosis. Obstet. Gynecol. 2012; 120; 1124–1131. - PubMed
-
- Rasool N, Fader AN, Seamon L et al. Stage I, grade 3 endometrioid adenocarcinoma of the endometrium: an analysis of clinical outcomes and patterns of recurrence. Gynecol. Oncol. 2010; 116; 10–14. - PubMed
-
- Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell 2011; 144; 646–674. - PubMed
-
- Concin N, Creutzberg CL, Vergote I et al. ESGO/ESTRO/ESP guidelines for the management of patients with endometrial carcinoma. Virchows Arch. 2021; 478; 153–190. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
