

Farnesyltransferase inhibition overcomes oncogene-addicted non-small cell lung cancer adaptive resistance to targeted therapies
- PMID: 38937474
- PMCID: PMC11211478
- DOI: 10.1038/s41467-024-49360-4
Farnesyltransferase inhibition overcomes oncogene-addicted non-small cell lung cancer adaptive resistance to targeted therapies
Abstract
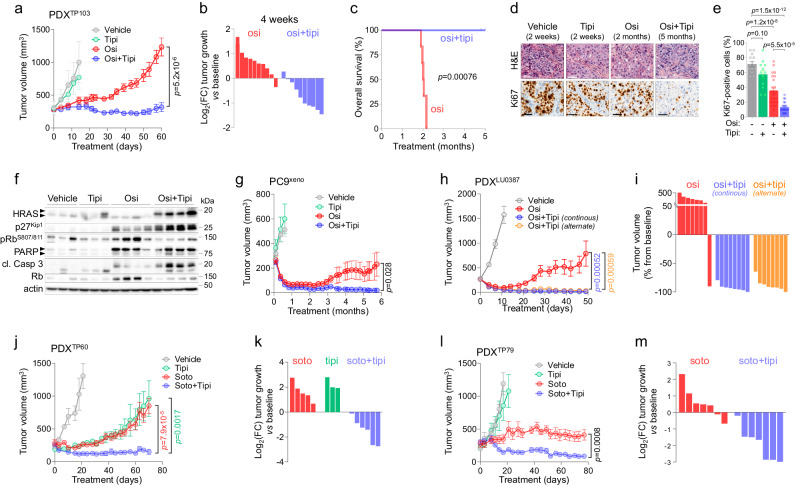
Drug-tolerance has emerged as one of the major non-genetic adaptive processes driving resistance to targeted therapy (TT) in non-small cell lung cancer (NSCLC). However, the kinetics and sequence of molecular events governing this adaptive response remain poorly understood. Here, we combine real-time monitoring of the cell-cycle dynamics and single-cell RNA sequencing in a broad panel of oncogenic addiction such as EGFR-, ALK-, BRAF- and KRAS-mutant NSCLC, treated with their corresponding TT. We identify a common path of drug adaptation, which invariably involves alveolar type 1 (AT1) differentiation and Rho-associated protein kinase (ROCK)-mediated cytoskeletal remodeling. We also isolate and characterize a rare population of early escapers, which represent the earliest resistance-initiating cells that emerge in the first hours of treatment from the AT1-like population. A phenotypic drug screen identify farnesyltransferase inhibitors (FTI) such as tipifarnib as the most effective drugs in preventing relapse to TT in vitro and in vivo in several models of oncogenic addiction, which is confirmed by genetic depletion of the farnesyltransferase. These findings pave the way for the development of treatments combining TT and FTI to effectively prevent tumor relapse in oncogene-addicted NSCLC patients.
© 2024. The Author(s).
Conflict of interest statement
O.C. reports research funding from Kura Oncology through a sponsored research contract. L.K. reports personal fees from Kura Oncology during the conduct of the study and personal fees from Kura Oncology outside the submitted work. FB is an employee and stockholder of Kura Oncology. JM reports personal fees/advisory board membership from Roche and Bristol Myers Squibb, and AstraZeneca, advisory board membership and research funding (institution), personal fees/advisory board membership from Pfizer, Novartis, Amgen, Takeda, Daiichi Sankyo, the healthcare business of Merck KGaA, Darmstadt, Germany, grants/funding (institution) from Roche/Genentech, Bristol Myers Squibb, Pierre Fabre and AstraZeneca outside the submitted work. L.P.A has leadership interest (board member) in ALTUM Sequencing and Genomica; has received honoraria for participation at meetings from Amgen Sanofi, AstraZeneca Spain, Bayer, Blueprint Medicines, Bristol Myers Squibb/Celgene, Daiichi Sankyo, Ipsen, Lilly, Merck Serono, Mirati Therapeutics, Novartis, Pfizer, PharmaMar, Roche/Genentech, Servier, and Takeda; speakers’ bureau from AstraZeneca, Bristol Myers Squibb, Merck Serono, MSD Oncology, Pfizer, and Roche/Genentech; research funding (via his institution) from AstraZeneca, Bristol Myers Squibb, Kura Oncology, MSD, Pfizer and PharmaMar; and travel and accommodation expenses from AstraZeneca, Bristol Myers Squibb/Celgene, MSD, Pfizer Roche/Genentech, and Takeda. L.P-A. also declares other relationships with Amgen, Ipsen, Merck, Novartis, Pfizer, Roche, Sanofi, and Servier (as sponsors of clinical trials), outside the submitted work. The remaining authors declare no conflict of interest.
Figures




References
-
- Rosell R, et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): a multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012;13:239–246. doi: 10.1016/S1470-2045(11)70393-X. - DOI - PubMed
MeSH terms
Substances
Grants and funding
- PJA2/Fondation ARC pour la Recherche sur le Cancer (ARC Foundation for Cancer Research)
- DEQ20170839117/Fondation pour la Recherche Médicale (Foundation for Medical Research in France)
- DEQ20170839117/Fondation pour la Recherche Médicale (Foundation for Medical Research in France)
- DEQ20170839117/Fondation pour la Recherche Médicale (Foundation for Medical Research in France)
- Inserm/Institut National de la Santé et de la Recherche Médicale (National Institute of Health and Medical Research)
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
